Conduit Ciara, Hong Wei, Martin Felicity, Thomas Benjamin, Lawrentschuk Nathan, Goad Jeremy, Grimison Peter, Ahmadi Nariman, Tran Ben, Lewin Jeremy
Department of Medical Oncology, Peter MacCallum Cancer Centre, Melbourne, VIC, Australia.
Sir Peter MacCallum Department of Oncology, The University of Melbourne, Parkville, VIC, Australia.
Front Oncol. 2022 Aug 17;12:931509. doi: 10.3389/fonc.2022.931509. eCollection 2022.
Post-chemotherapy retroperitoneal lymph node dissection (pcRPLND) for residual nodal masses is a critical component of care in metastatic testicular germ cell tumour (GCT). However, the procedure is not of therapeutic value in up to 50% of individuals in whom histopathology demonstrates post-treatment necrosis or fibrosis alone. Improved diagnostic tools and clinicopathologic features are needed to separate individuals who benefit from pcRPLND and avoid surgery in those who do not.
A prospectively registered meta-analysis of studies reporting clinicopathologic features associated with teratoma, GCT and/or necrosis/fibrosis at pcRPLND for metastatic non-seminoma GCT (NSGCT) was undertaken. We examined the effect of various clinicopathologic factors on the finding of necrosis/fibrosis at pcRPLND. The log odds ratios (ORs) of each association were pooled using random-effects models.
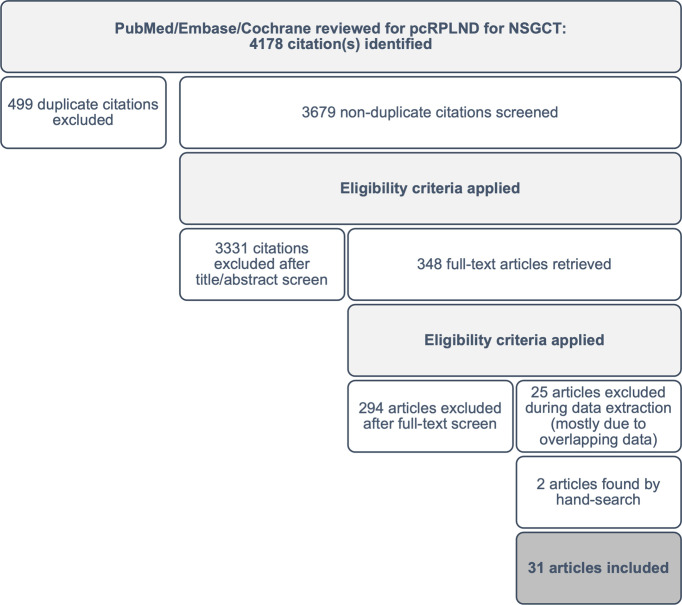
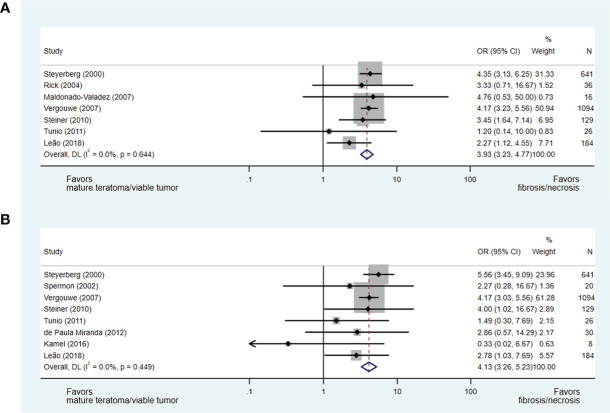
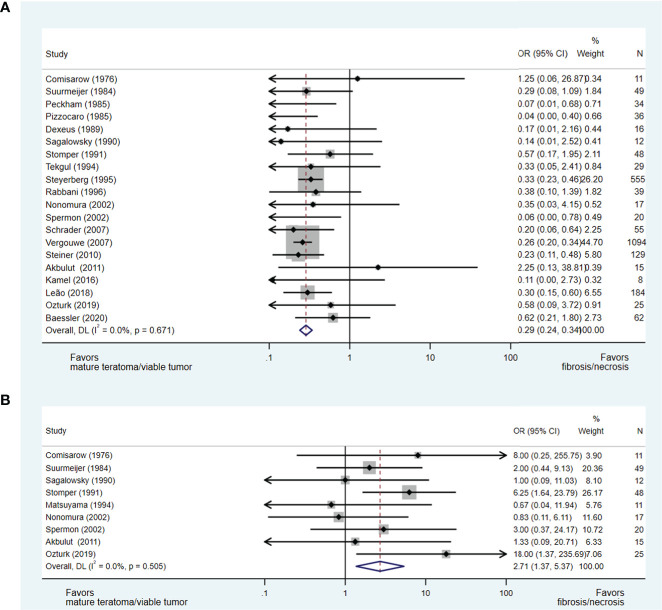
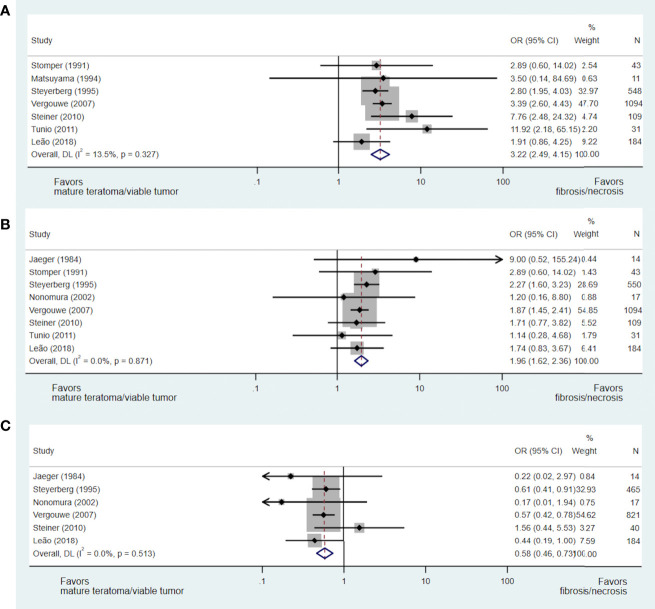
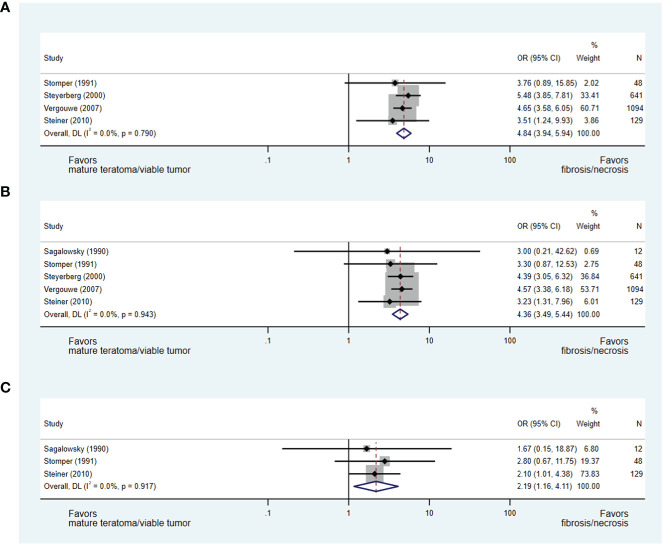
Using the initial search strategy, 4,178 potentially eligible abstracts were identified. We included studies providing OR relating to clinicopathologic factors predicting pcRPLND histopathology, or where individual patient-level data were available to permit the calculation of OR. A total of 31 studies evaluating pcRPLND histopathology in 3,390 patients were eligible for inclusion, including two identified through hand-searching the reference lists of eligible studies. The following were associated with the presence of necrosis/fibrosis at pcRPLND: absence of teratomatous elements in orchidectomy (OR 3.45, 95% confidence interval [CI] 2.94-4.17); presence of seminomatous elements at orchidectomy (OR 2.71, 95% CI 1.37-5.37); normal pre-chemotherapy serum bHCG (OR 1.96, 95% CI 1.62-2.36); normal AFP (OR 3.22, 95% CI 2.49-4.15); elevated LDH (OR 1.72, 95% CI 1.37-2.17); >50% change in mass during chemotherapy (OR 4.84, 95% CI 3.94-5.94); and smaller residual mass size (<2 cm 2: OR 3.93, 95% CI 3.23-4.77; <5 cm 5: OR 4.13, 95% CI 3.26-5.23).
In this meta-analysis, clinicopathologic features helped predict the presence of pcRPLND necrosis/fibrosis. Collaboration between centres that provide individual patient-level data is required to develop and validate clinical models and inform routine care to direct pcRPLND to individuals most likely to derive benefits.
https://www.crd.york.ac.uk/prospero/, identifier CRD42021279699.
对于残留淋巴结肿块进行化疗后腹膜后淋巴结清扫术(pcRPLND)是转移性睾丸生殖细胞肿瘤(GCT)治疗的关键组成部分。然而,在高达50%的组织病理学仅显示治疗后坏死或纤维化的个体中,该手术并无治疗价值。需要改进诊断工具和临床病理特征,以区分能从pcRPLND中获益的个体,并避免对无获益个体进行手术。
对报告转移性非精原细胞瘤性GCT(NSGCT)的pcRPLND时与畸胎瘤、GCT和/或坏死/纤维化相关的临床病理特征的研究进行前瞻性注册荟萃分析。我们研究了各种临床病理因素对pcRPLND时坏死/纤维化发现的影响。使用随机效应模型汇总每个关联的对数比值比(OR)。
采用初始检索策略,共识别出4178篇潜在合格摘要。我们纳入了提供与预测pcRPLND组织病理学的临床病理因素相关的OR的研究,或有个体患者水平数据可用于计算OR的研究。共有31项评估3390例患者pcRPLND组织病理学的研究符合纳入标准,包括通过手工检索合格研究的参考文献列表确定的2项研究。以下因素与pcRPLND时坏死/纤维化的存在相关:睾丸切除术中无畸胎瘤成分(OR 3.45,95%置信区间[CI] 2.94 - 4.17);睾丸切除术中存在精原细胞瘤成分(OR 2.71,95% CI 1.37 - 5.37);化疗前血清bHCG正常(OR 1.96,95% CI 1.62 - 2.36);甲胎蛋白(AFP)正常(OR 3.22,95% CI 2.49 - 4.15);乳酸脱氢酶(LDH)升高(OR 1.72,95% CI 1.37 - 2.17);化疗期间肿块变化>50%(OR 4.84,95% CI 3.94 - 5.94);残留肿块较小(<2 cm²:OR 3.93,95% CI 3.23 - 4.77;<5 cm⁵:OR 4.13,95% CI 3.26 - 5.23)。
在这项荟萃分析中,临床病理特征有助于预测pcRPLND坏死/纤维化的存在。需要提供个体患者水平数据的中心之间开展合作,以开发和验证临床模型,并为常规护理提供信息,从而将pcRPLND应用于最可能获益的个体。