Sjöö Mimmi, Berglund Annika, Sjöstrand Christina, Eriksson Einar E, Mazya Michael V
Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden.
Department of Neurology, Karolinska University Hospital, Stockholm, Sweden.
Front Neurol. 2022 Aug 18;13:939618. doi: 10.3389/fneur.2022.939618. eCollection 2022.
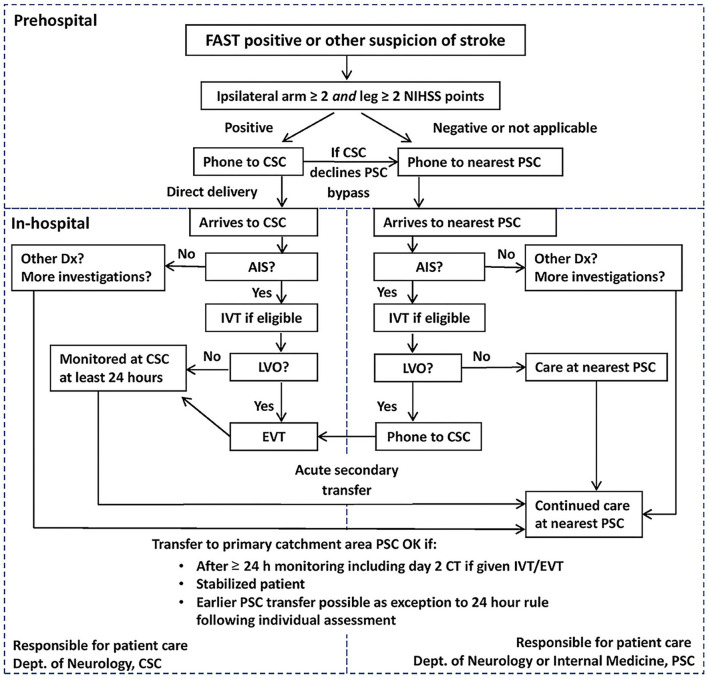
In 2017, Stockholm implemented a new prehospital stroke triage system (SSTS) directing patients with a likely indication for thrombectomy to the regional comprehensive stroke center (CSC) based on symptom severity and teleconsultation with a physician. In Stockholm, 44% of patients with prehospital code stroke have stroke mimics. Inadvertent triage of stroke mimics to the CSC could lead to inappropriate resource utilization.
To compare the characteristics between (1) triage-positive stroke mimics and stroke (TP mimics and TP stroke) and (2) triage-negative stroke mimics and stroke (TN mimics and TN stroke) and to (3) compare the distribution of stroke mimic diagnoses between triage-positive and triage-negative cases.
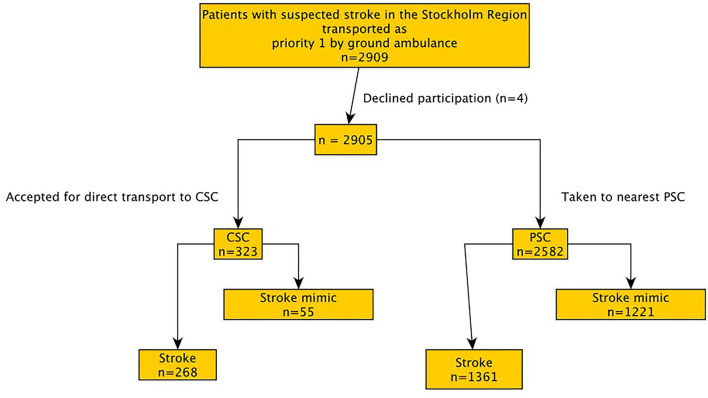
This prospective observational study collected data from October 2017 to October 2018, including 2,905 patients with suspected stroke who were transported by code-stroke ambulance to a Stockholm regional hospital. Patients directed to the CSC were defined as triage-positive. Those directed to the nearest stroke center were defined as triage-negative.
Compared to individuals with TP stroke ( = 268), those with TP mimics ( = 55, median 64 vs. 75 years, < 0.001) were younger and had lower NIHSS score (median 7 vs. 15, < 0.001). Similarly, those with TN mimics ( = 1,221) were younger than those with TN stroke (n = 1,361, median 73 vs. 78 years, < 0.001) and had lower NIHSS scores (median 2 vs. 4, < 0.001). Functional paresis was more common in those with TP mimics than in those with TN mimics, 18/55 (32.7%) vs. 82/1,221 (6.7%), < 0.001. Systemic infection was less common in those with TP mimics than in those with TN mimics, 1/55 (1.8%) vs. 160/1,221 (13.1%), < 0.011. There was a trend toward "syncope, hypotension, or other cardiovascular diagnosis" being less common in those with TP mimics than in those with TN mimics, 1/55 (1.8%) vs. 118/1,221 (9.7%), < 0.055.
In the SSTS, those with triage-positive and triage-negative stroke mimics were younger and had less severe symptoms than patients with stroke. All patients with TP mimics who had hemiparesis but overall exhibited less severe symptoms against true stroke but more severe symptoms than those with TN mimics were triaged to the nearest hospital. Over-triage of functional paresis to the CSC was relatively common. Meanwhile, a large majority of cases with minor symptoms caused by stroke mimics was triaged correctly by the SSTS to the nearest stroke center.
2017年,斯德哥尔摩实施了一种新的院前卒中分诊系统(SSTS),该系统根据症状严重程度并通过与医生进行远程会诊,将可能适合进行血栓切除术的患者送往区域综合卒中中心(CSC)。在斯德哥尔摩,44%的院前卒中编码患者存在卒中模拟症状。将存在卒中模拟症状的患者误分诊至CSC可能导致资源利用不当。
比较(1)分诊阳性的卒中模拟症状患者与卒中患者(TP模拟症状患者与TP卒中患者)之间的特征,(2)分诊阴性的卒中模拟症状患者与卒中患者(TN模拟症状患者与TN卒中患者)之间的特征,以及(3)比较分诊阳性和分诊阴性病例中卒中模拟症状诊断的分布情况。
这项前瞻性观察性研究收集了2017年10月至2018年10月的数据,包括2905例疑似卒中患者,这些患者由卒中编码救护车转运至斯德哥尔摩地区医院。被送往CSC的患者被定义为分诊阳性。被送往最近的卒中中心的患者被定义为分诊阴性。
与TP卒中患者(n = 268)相比,TP模拟症状患者(n = 55,中位年龄64岁对75岁,P < 0.001)更年轻,美国国立卫生研究院卒中量表(NIHSS)评分更低(中位评分7分对15分,P < 0.001)。同样,TN模拟症状患者(n = 1221)比TN卒中患者(n = 1361,中位年龄73岁对78岁,P < 0.001)更年轻,NIHSS评分更低(中位评分2分对4分,P < 0.001)。功能性轻瘫在TP模拟症状患者中比在TN模拟症状患者中更常见,分别为18/55(32.7%)对82/1221(6.7%),P < 0.001。全身性感染在TP模拟症状患者中比在TN模拟症状患者中更少见,分别为1/55(1.8%)对160/1221(13.1%),P < 0.011。“晕厥、低血压或其他心血管诊断”在TP模拟症状患者中比在TN模拟症状患者中似乎更少见,分别为1/55(1.8%)对118/1221(9.7%),P < 0.055。
在SSTS中,分诊阳性和分诊阴性的卒中模拟症状患者比卒中患者更年轻,症状也不那么严重。所有存在偏瘫的TP模拟症状患者总体上与真正的卒中相比症状较轻,但比重症模拟症状患者症状更严重,他们被分诊到了最近的医院。将功能性轻瘫过度分诊至CSC相对常见。同时,SSTS将绝大多数由卒中模拟症状引起的轻微症状病例正确分诊到了最近的卒中中心。