Division of Infectious Diseases, Department of Internal Medicine and AIDS Research Institute, Yonsei University College of Medicine, Yonsei University Health System, Seoul, South Korea, 50-1, Yonsei-ro, Seodaemun-gu, 03722.
Sci Rep. 2022 Sep 5;12(1):15059. doi: 10.1038/s41598-022-19405-z.
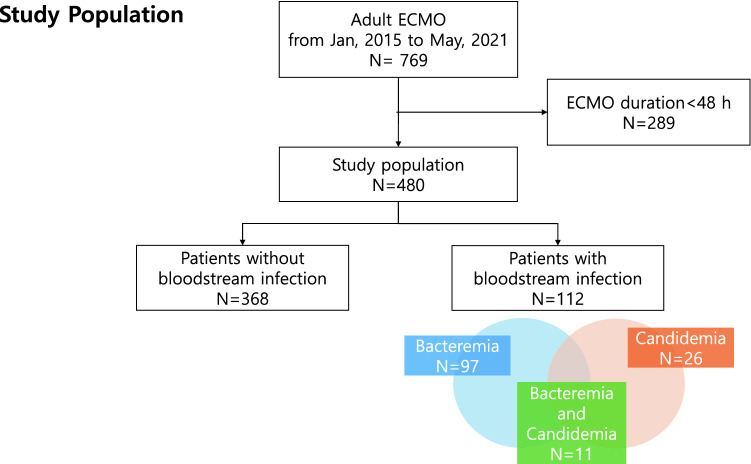
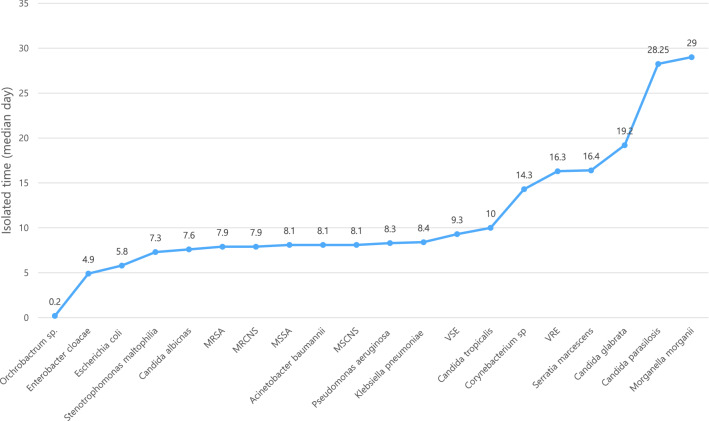
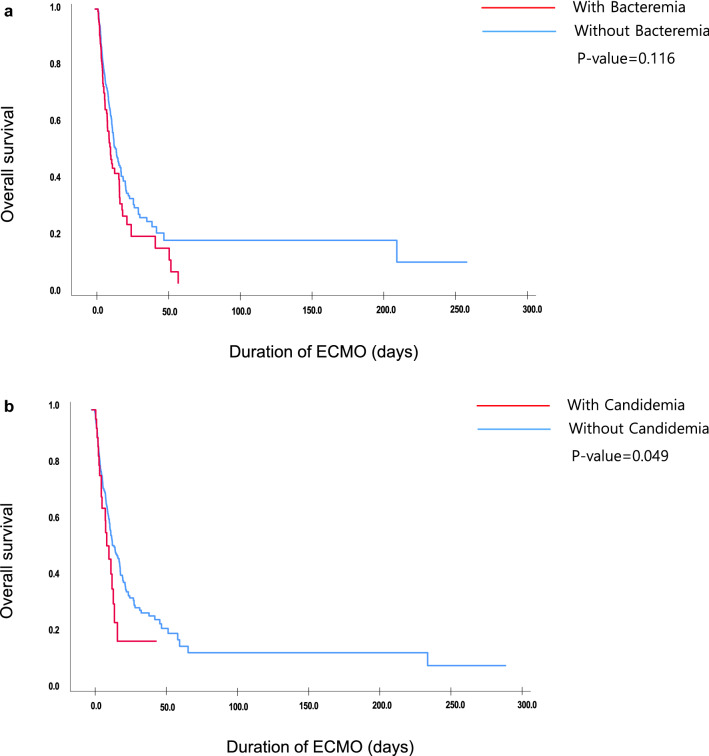
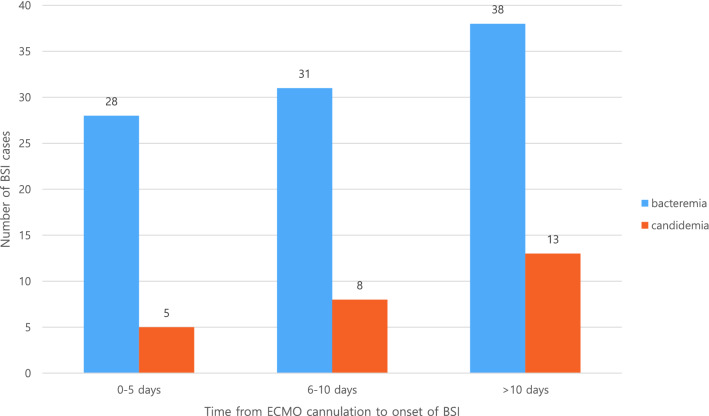
Extracorporeal membrane oxygenation (ECMO) provides hemodynamic and oxygenation support to critically ill patients. Due to multiple catheter cannulations, patients on ECMO are vulnerable to bloodstream infections (BSIs). We aimed to investigate the incidence, clinical characteristics, risk factors, and microorganisms associated with BSIs during ECMO. This single-center retrospective cohort study was conducted between January 2015 and May 2021. Patients aged 18 years or older with an ECMO duration of > 48 h for cardiogenic or respiratory support were included in the study. Patients who developed bacteremia or candidemia from 12 h after ECMO cannulation to 7 days after de-cannulation were included. The clinical factors between non-BSI and BSI were compared, along with an analysis of the risk factors associated with BSI during ECMO. A total of 480 patients underwent ECMO for cardiogenic shock (n = 267, 55.6%) or respiratory failure (n = 213, 44.4%) during the study period. The incidence was 20.0 episodes per 1000 ECMO-days. Approximately 20.2% (97/480) and 5.4% (26/480) of the patients developed bacteremia and candidemia, respectively. The median numbers of days of BSI development were 8.00 days for bacteremia and 11.0 days for candidemia. The most common pathogens were methicillin-resistant coagulase-negative staphylococci (n = 24), followed by vancomycin-resistant Enterococcus (n = 21). Multivariable logistic analysis demonstrated that hemodialysis (odds ratio [OR] 2.647, p < 0.001), veno-arterial-venous mode (OR 1.911, p = 0.030), and total ECMO duration (OR 1.030, p = 0.007) were significant risk factors for bacteremia. The total ECMO duration was the only risk factor associated with candidemia (OR 1.035, p = 0.010). The mortality rate was significantly higher in the bacteremia (57.7%) and candidemia (69.2%) groups than that in the non-BSI group (43.6%). BSI is a common complication of patients receiving ECMO support and is associated with poor clinical outcomes. Determining the type of frequently isolated organisms and the median onset time of BSI would help in the selection of appropriate prophylactic antibiotics or antifungal agents.
体外膜肺氧合(ECMO)为危重症患者提供血液动力学和氧合支持。由于需要多次导管插管,接受 ECMO 治疗的患者易发生血流感染(BSI)。我们旨在研究 ECMO 期间 BSI 的发生率、临床特征、危险因素和相关微生物。这是一项单中心回顾性队列研究,于 2015 年 1 月至 2021 年 5 月进行。研究纳入 ECMO 持续时间超过 48 小时,用于治疗心源性或呼吸支持的年龄在 18 岁或以上的患者。从 ECMO 插管后 12 小时至拔管后 7 天发生菌血症或念珠菌血症的患者也纳入研究。比较非 BSI 和 BSI 患者的临床因素,并分析 ECMO 期间与 BSI 相关的危险因素。在研究期间,共有 480 名患者因心源性休克(n=267,55.6%)或呼吸衰竭(n=213,44.4%)接受 ECMO 治疗。BSI 的发生率为每 1000 个 ECMO 天 20.0 个。大约 20.2%(97/480)和 5.4%(26/480)的患者分别发生菌血症和念珠菌血症。BSI 发生的中位天数为菌血症 8.00 天,念珠菌血症 11.0 天。最常见的病原体是耐甲氧西林凝固酶阴性葡萄球菌(n=24),其次是万古霉素耐药肠球菌(n=21)。多变量逻辑分析表明,血液透析(比值比[OR]2.647,p<0.001)、动静脉-静脉模式(OR 1.911,p=0.030)和总 ECMO 持续时间(OR 1.030,p=0.007)是菌血症的显著危险因素。总 ECMO 持续时间是与念珠菌血症相关的唯一危险因素(OR 1.035,p=0.010)。菌血症(57.7%)和念珠菌血症(69.2%)组的死亡率明显高于非 BSI 组(43.6%)。BSI 是接受 ECMO 支持患者的常见并发症,与不良临床结局相关。确定经常分离的生物体类型和 BSI 的中位发病时间有助于选择合适的预防性抗生素或抗真菌药物。