Department of Ophthalmology, Faculty of Medicine, Akdeniz University, Pınarbaşı Mah. Akdeniz Üniversitesi Tıp Fakültesi Hastanesi, Antalya, Turkey.
Department of Microbiology, Faculty of Medicine, Akdeniz University, Antalya, Turkey.
J Med Case Rep. 2022 Sep 7;16(1):340. doi: 10.1186/s13256-022-03566-6.
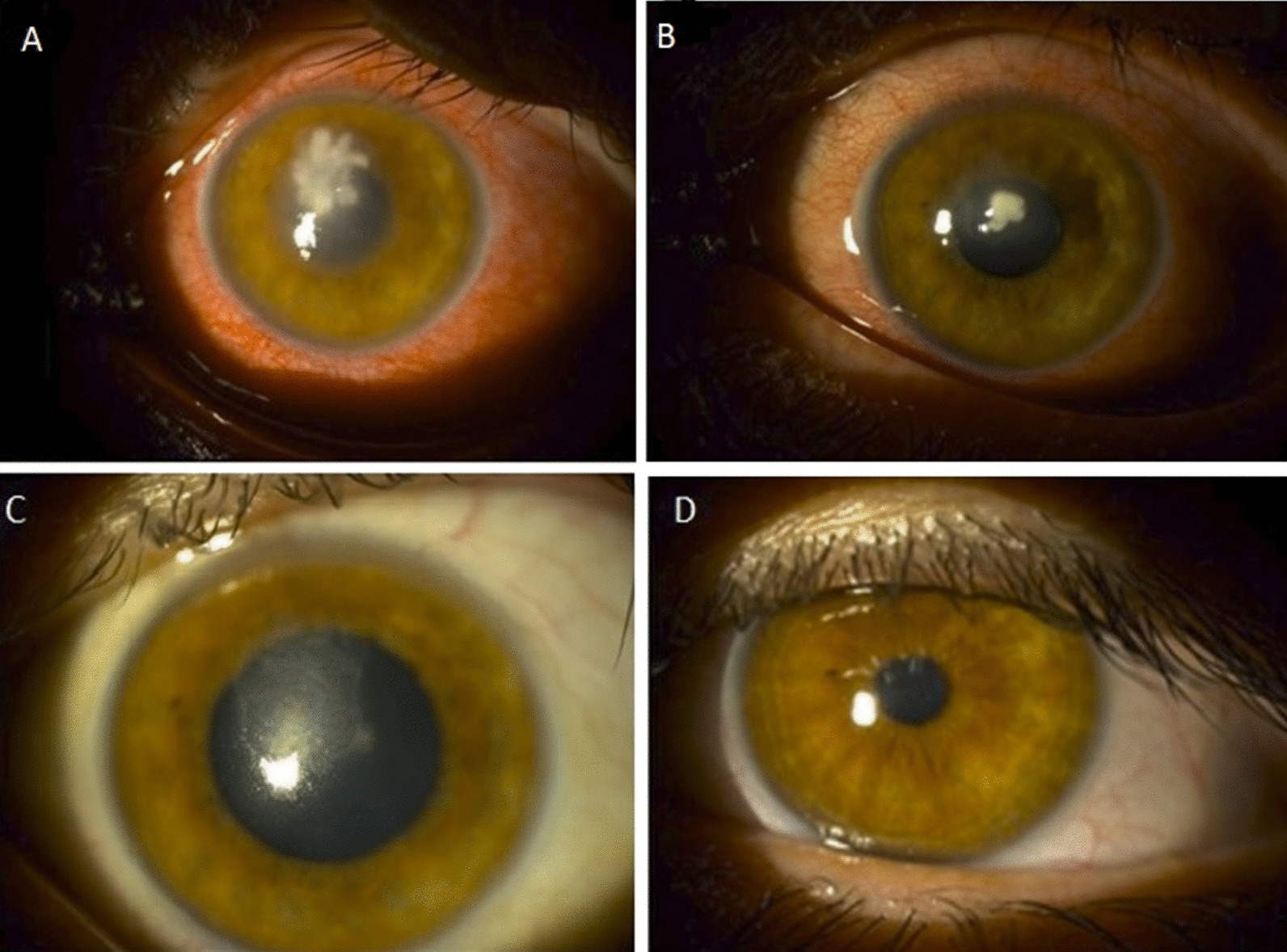
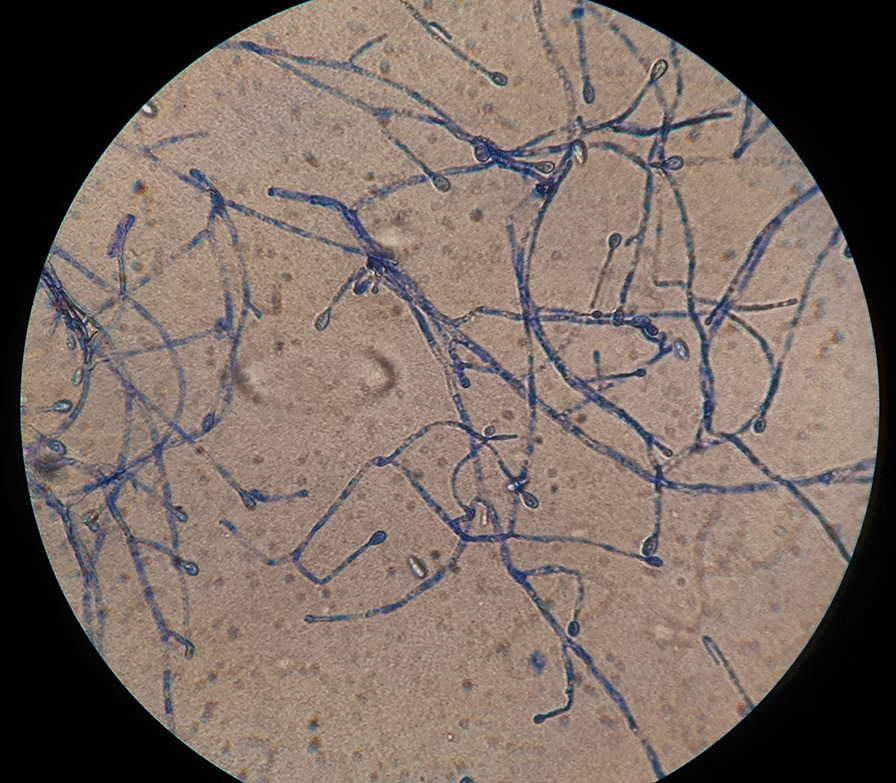
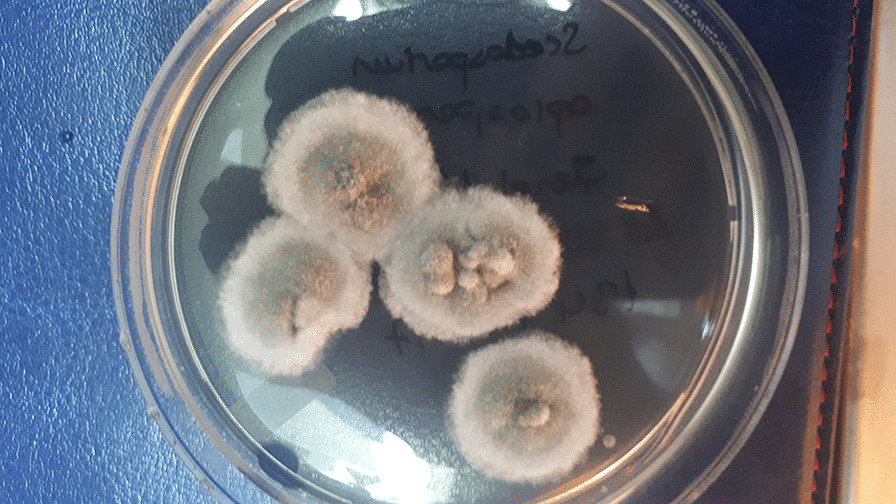
We present a case of fungal keratitis caused by Scedosporium apiospermum, which is a rare agent. Case description A 34-year-old Caucasian male patient was admitted to our clinic with complaints of pain and blurred vision in the left eye. The patient had a history of wearing contact lenses for 3 years. According to the Snellen chart, the patient's visual acuity was 20/20 and counting fingers at 30 cm, for right and left eyes, respectively. A 3 × 3 mm corneal abscess at the center of the cornea with hypopyon in the patient's left eye was observed. After the patient was hospitalized, fortified gentamicin and fortified cefazolin drops were started 24 times per day. Intravenous fluconazole 1 × 800 mg loading, 1 × 400 mg maintenance dose, intravenous vancomycin 4 × 500 mg and intravenous cefoperazone + sulbactam 2 × 2 g treatments were started. We observed S. apiospermum in the corneal scraping sample, which the identification was performed by combined phenotypic characteristics and matrix-assisted laser-desorption ionization time-of-flight mass spectrometry on the sixth day of treatment. The drops were revised as fortified vancomycin, ceftazidime, and voriconazole drops 24 times per day. Intravenous voriconazole 2 × 6 mg/kg loading and 2 × 4 mg/kg maintenance dose treatments were started. Three weeks later, left eye visual acuity increased to 20/40, and the corneal abscess regressed. On second-year follow-up, his visual acuity increased to 20/25 for the left eye and the cornea was transparent.
Scedosporium group is an opportunistic filamentous fungus that is very rarely seen and causes severe keratitis infections. In the literature, to the best of our knowledge, three cases of keratitis due to S. apiospermum after contact lenses were reported, and all were treated with penetrating keratoplasty. In this case, unlike the others, only medical treatment was applied. In cases with suspected fungal keratitis, medical treatment should be started without waiting for the culture result, the findings should be followed and penetrating keratoplasty should be performed in the case of no response to treatment.
我们报告了一例由枝顶孢属真菌引起的真菌性角膜炎,该真菌较为罕见。
一名 34 岁的白人男性因左眼疼痛和视力模糊到我院就诊。患者有 3 年佩戴隐形眼镜的病史。根据 Snellen 图表,患者右眼视力为 20/20,左眼视力为 30cm 处可识别手指,左眼有 3×3mm 角膜中央脓肿,伴有前房积脓。患者住院后,开始每天 24 次强化庆大霉素和头孢唑林滴眼治疗。静脉注射氟康唑 1×800mg 负荷量,1×400mg 维持量,静脉注射万古霉素 4×500mg 和头孢哌酮+舒巴坦 2×2g,第 6 天在角膜刮片样本中观察到枝顶孢属真菌,治疗第 6 天通过联合表型特征和基质辅助激光解吸电离飞行时间质谱鉴定为枝顶孢属真菌。滴眼剂修订为每天 24 次强化万古霉素、头孢他啶和伏立康唑滴眼治疗。静脉注射伏立康唑 2×6mg/kg 负荷量和 2×4mg/kg 维持量。3 周后,左眼视力提高至 20/40,角膜脓肿消退。在第二年的随访中,左眼视力增加到 20/25,角膜透明。
枝顶孢属是一种机会性丝状真菌,非常罕见,可引起严重的角膜炎感染。在文献中,据我们所知,有三例因接触镜后枝顶孢属角膜炎的报道,均行穿透性角膜移植术。在本例中,与其他病例不同,仅进行了药物治疗。对于疑似真菌性角膜炎的病例,应在等待培养结果的同时开始药物治疗,应密切关注病情变化,并在治疗无效时进行穿透性角膜移植术。