University of Pittsburgh, Pittsburgh, PA, USA.
Carnegie Mellon University, Pittsburgh, PA, USA.
Mol Psychiatry. 2022 Dec;27(12):5096-5112. doi: 10.1038/s41380-022-01757-7. Epub 2022 Sep 7.
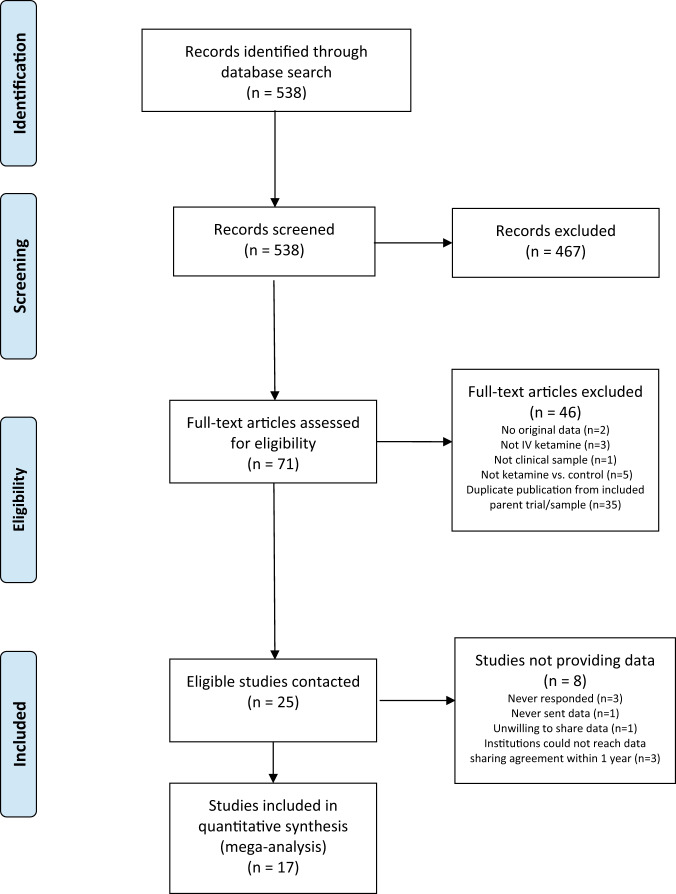
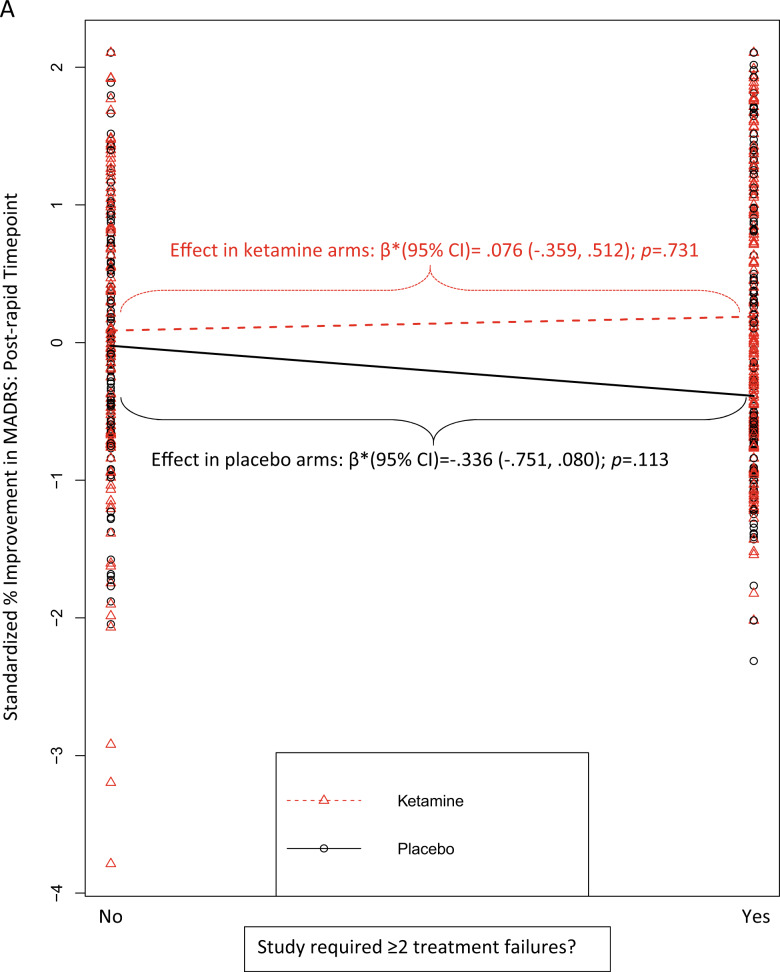
Depression is disabling and highly prevalent. Intravenous (IV) ketamine displays rapid-onset antidepressant properties, but little is known regarding which patients are most likely to benefit, limiting personalized prescriptions. We identified randomized controlled trials of IV ketamine that recruited individuals with a relevant psychiatric diagnosis (e.g., unipolar or bipolar depression; post-traumatic stress disorder), included one or more control arms, did not provide any other study-administered treatment in conjunction with ketamine (although clinically prescribed concurrent treatments were allowable), and assessed outcome using either the Montgomery-Åsberg Depression Rating Scale or the Hamilton Rating Scale for Depression (HRSD-17). Individual patient-level data for at least one outcome was obtained from 17 of 25 eligible trials [pooled n = 809]. Rates of participant-level data availability across 33 moderators that were solicited from these 17 studies ranged from 10.8% to 100% (median = 55.6%). After data harmonization, moderators available in at least 40% of the dataset were tested sequentially, as well as with a data-driven, combined moderator approach. Robust main effects of ketamine on acute [24-hours; β*(95% CI) = 0.58 (0.44, 0.72); p < 0.0001] and post-acute [7 days; β*(95% CI) = 0.38 (0.23, 0.54); p < 0.0001] depression severity were observed. Two study-level moderators emerged as significant: ketamine effects (relative to placebo) were larger in studies that required a higher degree of previous treatment resistance to federal regulatory agency-approved antidepressant medications (≥2 failed trials) for study entry; and in studies that used a crossover design. A comprehensive data-driven search for combined moderators identified statistically significant, but modest and clinically uninformative, effects (effect size r ≤ 0.29, a small-medium effect). Ketamine robustly reduces depressive symptoms in a heterogeneous range of patients, with benefit relative to placebo even greater in patients more resistant to prior medications. In this largest effort to date to apply precision medicine approaches to ketamine treatment, no clinical or demographic patient-level features were detected that could be used to guide ketamine treatment decisions.Review Registration: PROSPERO Identifier: CRD42021235630.
抑郁症具有致残性且普遍存在。静脉注射(IV)氯胺酮显示出快速抗抑郁的特性,但对于哪些患者最有可能受益知之甚少,限制了个性化处方。我们确定了招募具有相关精神诊断(例如,单相或双相抑郁症;创伤后应激障碍)的个体的随机对照试验,这些试验包括一个或多个对照组,不提供任何其他由研究人员给予的与氯胺酮联合治疗(尽管允许临床规定的同时治疗),并使用蒙哥马利-Åsberg 抑郁评定量表或汉密尔顿抑郁评定量表(HRSD-17)评估结果。从 25 项符合条件的试验中获得了至少一项结果的 17 项个体患者水平数据[汇总 n=809]。从这 17 项研究中征求了 33 个调节因素的参与者水平数据可用性,其范围为 10.8%至 100%(中位数=55.6%)。在数据协调后,以至少 40%的数据集提供的调节因素进行了依次测试,以及采用数据驱动的综合调节因素方法进行了测试。氯胺酮对急性[约 24 小时;β*(95%CI)=0.58(0.44,0.72);p<0.0001]和亚急性[约 7 天;β*(95%CI)=0.38(0.23,0.54);p<0.0001]抑郁严重程度的影响是稳健的。出现了两个研究水平的调节因素:对于进入研究需要更高程度的先前对联邦监管机构批准的抗抑郁药物(≥2 项失败试验)治疗的抵抗性的研究;以及使用交叉设计的研究,氯胺酮的作用(相对于安慰剂)更大。对综合调节因素的全面数据驱动搜索发现了具有统计学意义但适度且临床无意义的影响(效应大小 r≤0.29,小-中效应)。氯胺酮在各种患者中稳健地减轻抑郁症状,与安慰剂相比,对先前药物更具耐药性的患者的益处更大。在迄今为止最大的努力中,将精准医学方法应用于氯胺酮治疗,没有检测到可以用于指导氯胺酮治疗决策的临床或人口统计学患者水平特征。
PROSPERO 标识符:CRD42021235630。