The Royal's Institute of Mental Health Research, 1145 Carling Avenue, Ottawa, ON, K1Z 7K4, Canada.
Department of Psychiatry, University of Ottawa, 1145 Carling Avenue, Ottawa, ON, K1Z 7K4, Canada.
BMC Psychiatry. 2020 Jun 2;20(1):268. doi: 10.1186/s12888-020-02672-3.
Recent evidence underscores the utility of rapid-acting antidepressant interventions, such as ketamine, in alleviating symptoms of major depressive episodes (MDE). However, to date, there have been limited head-to-head comparisons of intravenous (IV) ketamine infusions with other antidepressant treatment strategies in large randomized trials. This study protocol describes an ongoing multi-centre, prospective, randomized, crossover, non-inferiority trial comparing acute treatment of individuals meeting diagnostic criteria for a major depressive episode (MDE) with ketamine and electroconvulsive therapy (ECT) on efficacy, speed of therapeutic effects, side effects, and health care resource utilization. A secondary aim is to compare a 6-month maintenance strategy for ketamine responders to standard of care ECT maintenance. Finally, through the measurement of clinical, cognitive, neuroimaging, and molecular markers we aim to establish predictors and moderators of treatment response as well as treatment-elicited effects on these outcomes.
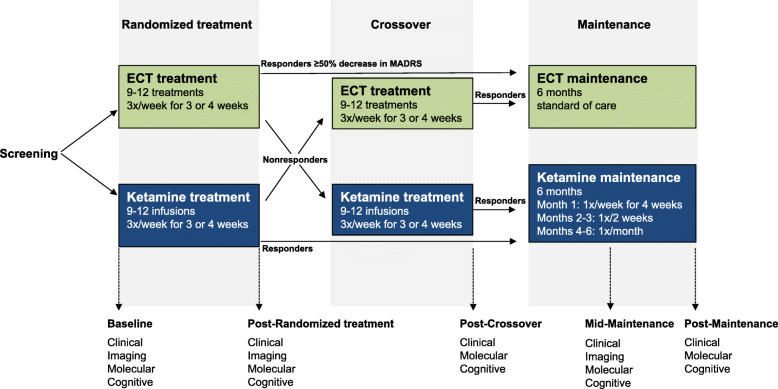
Across four participating Canadian institutions, 240 patients with major depressive disorder or bipolar disorder experiencing a MDE are randomized (1:1) to a course of ECT or racemic IV ketamine (0.5 mg/kg) administered 3 times/week for 3 or 4 weeks. Non-responders (< 50% improvement in Montgomery-Åsberg Depression Rating Scale [MADRS] scores) crossover to receive the alternate treatment. Responders during the randomization or crossover phases then enter the 6-month maintenance phase during which time they receive clinical assessments at identical intervals regardless of treatment arm. ECT maintenance follows standard of care while ketamine maintenance involves: weekly infusions for 1 month, then bi-weekly infusions for 2 months, and finally monthly infusions for 3 months (returning to bi-weekly in case of relapse). The primary outcome measure is change in MADRS scores after randomized treatment as assessed by raters blind to treatment modality.
This multi-centre study will help identify molecular, imaging, and clinical characteristics of patients with treatment-resistant and/or severe MDEs who would benefit most from either type of therapeutic strategy. In addition to informing clinical practice and influencing health care delivery, this trial will add to the robust platform and database of CAN-BIND studies for future research and biomarker discovery.
ClinicalTrials.gov identifier NCT03674671. Registered September 17, 2018.
最近的证据强调了快速作用抗抑郁药干预的效用,例如氯胺酮,可缓解重度抑郁发作(MDE)的症状。然而,迄今为止,在大型随机试验中,静脉内(IV)氯胺酮输注与其他抗抑郁治疗策略的头对头比较有限。本研究方案描述了一项正在进行的多中心、前瞻性、随机、交叉、非劣效性试验,比较了符合重度抑郁发作(MDE)诊断标准的个体的急性治疗,使用氯胺酮和电惊厥疗法(ECT)的疗效、治疗效果的速度、副作用和医疗资源利用。次要目标是比较氯胺酮反应者的 6 个月维持治疗策略与标准护理 ECT 维持治疗。最后,通过测量临床、认知、神经影像学和分子标志物,我们旨在确定治疗反应的预测因子和调节剂以及治疗对这些结果的影响。
在四个参与的加拿大机构中,240 名患有重度抑郁症或双相情感障碍且正在经历 MDE 的患者随机(1:1)接受 ECT 或外消旋 IV 氯胺酮(0.5mg/kg)治疗,每周 3 次,持续 3 或 4 周。未应答者(<50%的蒙哥马利-阿斯伯格抑郁评定量表[MADRS]评分改善)交叉接受另一种治疗。随机或交叉阶段的应答者然后进入 6 个月的维持期,在此期间,无论治疗组如何,他们都以相同的间隔接受临床评估。ECT 维持采用标准护理,而氯胺酮维持涉及:1 个月每周输注,然后 2 个月每两周输注,最后 3 个月每月输注(如果复发则每两周一次)。主要结局测量指标是盲法评估治疗方式后的 MADRS 评分变化。
这项多中心研究将有助于确定治疗抵抗和/或重度 MDE 患者的分子、影像学和临床特征,这些患者最适合哪种治疗策略。除了为临床实践提供信息并影响医疗保健的提供外,该试验还将为 CAN-BIND 研究的强大平台和数据库增添力量,以进行未来的研究和生物标志物发现。
ClinicalTrials.gov 标识符 NCT03674671。注册日期为 2018 年 9 月 17 日。