Division of Gastroenterology, Department of Internal Medicine, Kobe University Graduate School of Medicine, 7-5-2 Kusunoki-cho, Chuo-ku, Kobe, Hyogo, 650-0017, Japan.
Division of Gastroenterology, Department of Internal Medicine, Kobe University Graduate School of Medicine, 7-5-2 Kusunoki-cho, Chuo-ku, Kobe, 650-0017, Japan.
Sci Rep. 2022 Sep 7;12(1):15134. doi: 10.1038/s41598-022-19439-3.
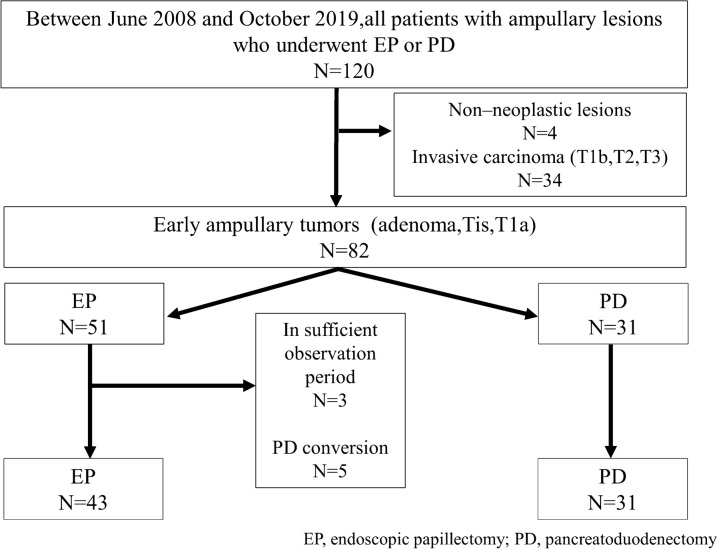
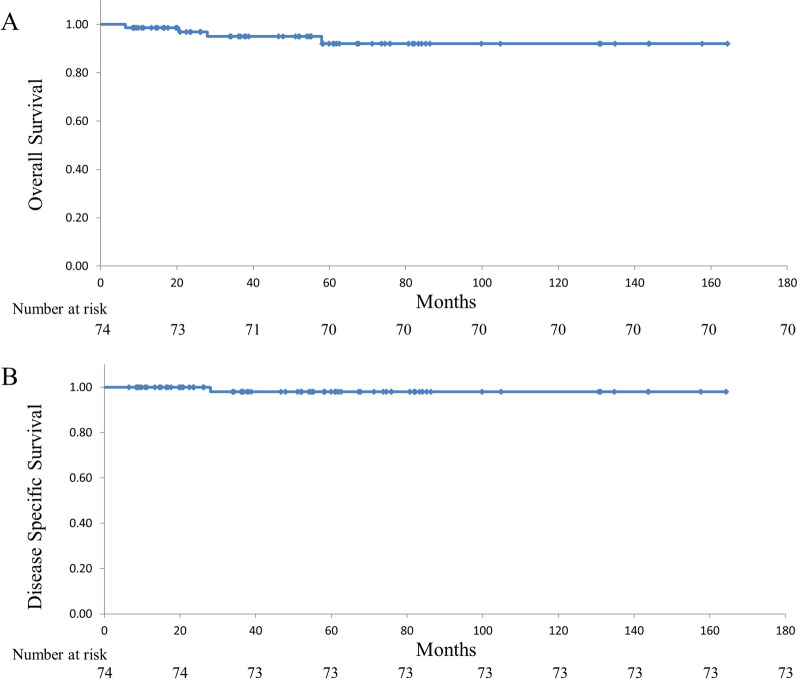
Endoscopic papillectomy for early ampullary tumors is considered a minimally invasive and useful alternative to pancreatoduodenectomy; however, its indications remain unclear. This study aimed to clarify the advantages of endoscopic papillectomy by investigating the clinical outcomes of patients who underwent endoscopic papillectomy or pancreatoduodenectomy for early ampullary tumors. Patients diagnosed with early ampullary tumors (adenoma, Tis, T1a) who underwent endoscopic papillectomy or pancreatoduodenectomy between June 2008 and October 2019 were included, and their clinical outcomes were analyzed. Seventy-four patients (34 patients with adenomas and 40 patients with adenocarcinomas) were divided into two groups, namely endoscopic papillectomy (n = 43) and pancreatoduodenectomy (n = 31). The estimated 5-year overall survival rate of all early ampullary tumors was 92%. Complete resection rate was significantly lower for endoscopic papillectomy patients versus pancreatoduodenectomy patients (48.8% vs. 100%; p < 0.001). Recurrence was more common in the endoscopic papillectomy group compared to the pancreatoduodenectomy group (16.3% vs. 3.2%; p = 0.128), but all recurrences were controllable by endoscopic treatment. The median length of hospital stay for the endoscopic papillectomy group was significantly shorter compared to the endoscopic papillectomy group (11 days vs. 42 days; p < 0.001). The Comprehensive Complication Index was significantly lower in the endoscopic papillectomy group compared to the pancreatoduodenectomy group (14.8 vs 22.6%; p = 0.002). Endoscopic papillectomy for early ampullary tumors is useful and may be an alternative treatment for pancreatoduodenectomy in selected cases.
内镜乳头肿瘤切除术被认为是一种微创且有效的替代胰十二指肠切除术的方法;然而,其适应证仍不明确。本研究旨在通过研究接受内镜乳头肿瘤切除术或胰十二指肠切除术的早期壶腹肿瘤患者的临床结果来阐明内镜乳头肿瘤切除术的优势。
纳入 2008 年 6 月至 2019 年 10 月期间接受内镜乳头肿瘤切除术或胰十二指肠切除术治疗的早期壶腹肿瘤(腺瘤、Tis、T1a)患者,并分析其临床结果。74 例患者(34 例腺瘤和 40 例腺癌)分为两组,即内镜乳头肿瘤切除术(n=43)和胰十二指肠切除术(n=31)。所有早期壶腹肿瘤的估计 5 年总生存率为 92%。内镜乳头肿瘤切除术患者的完全切除率明显低于胰十二指肠切除术患者(48.8% vs. 100%;p<0.001)。内镜乳头肿瘤切除术组的复发率高于胰十二指肠切除术组(16.3% vs. 3.2%;p=0.128),但所有复发均可以通过内镜治疗控制。内镜乳头肿瘤切除术组的中位住院时间明显短于胰十二指肠切除术组(11 天 vs. 42 天;p<0.001)。内镜乳头肿瘤切除术组的综合并发症指数明显低于胰十二指肠切除术组(14.8 比 22.6%;p=0.002)。
内镜乳头肿瘤切除术治疗早期壶腹肿瘤是有用的,在某些情况下可能是胰十二指肠切除术的替代治疗方法。