Uganda Public Health Fellowship Program, Kampala, Uganda.
Ministry of Health Uganda, Kampala, Uganda.
BMC Public Health. 2022 Sep 7;22(1):1694. doi: 10.1186/s12889-022-14077-w.
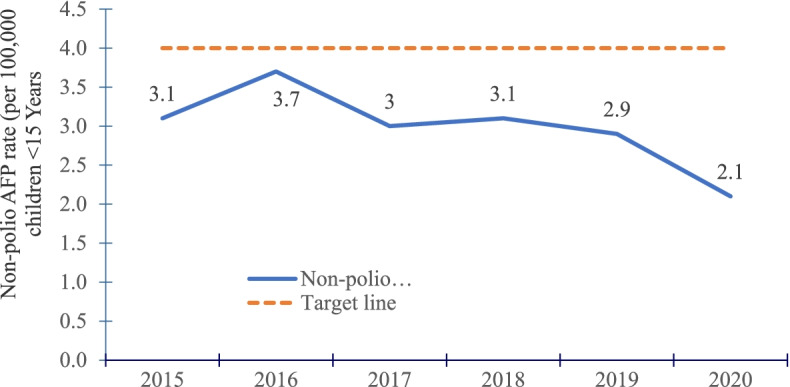
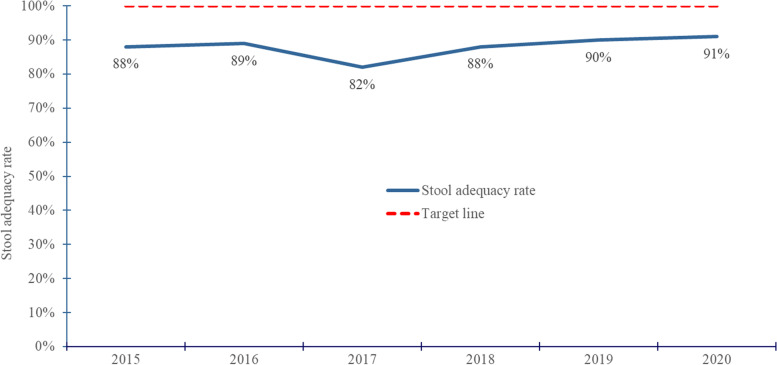
Polio is disease caused by poliovirus which can in turn cause irreversible paralytic disease, presenting as Acute Flaccid Paralysis (AFP). A sensitive AFP surveillance system, in which all reported AFP cases are evaluated, first to determine if they are true AFP cases or not, is key for tracking polio eradication. True AFP cases are then later categorized as polio AFP or non-polio AFP (NPAFP) cases. Sensitivity is defined by meeting an annual NPAFP rate/100,000 population < 15 years of ≥ 4/100,000, and an annual stool adequacy (SA) rate of ≥ 80%. We describe Uganda's AFP surveillance performance between 2015-2020, based on the WHO-recommended indicators, including; NPAFP and stool adequacy rate.
We performed a descriptive analysis of national AFP surveillance data, 2015-2020 obtained from ministry of health. We evaluated proportion of reported AFP cases that were true AFP, and changes in NPAFP and stool adequacy (SA) rate over the study period. We evaluated the trends in achieving the targeted NPAFP and SA rates from 2015-2020. We used QGIS to illustrate patterns in NPAFP and SA rates across districts and subregions.
Among 3,605 AFP cases reported and investigated countrywide from 2015-2020, 3,475 (96%) were true AFP cases. All the true AFP cases were non-polio related. District reporting was near-complete (97-100% each year). Overall, the mean NPAFP rate declined from 3.1/100,000 in 2015 to 2.1/100,000 in 2020. Less than 40% of districts met the NPAFP target rate in all years. The proportion of districts achieving the NPAFP target rate of ≥ 4/100,000 significantly declined from 35% in 2015 to 20% in 2020. The mean annual SA rate nationally was 88% from 2015-2020. Only 66% of districts achieved the SA target rate of ≥ 80% in the study period. The proportion of districts with SA rate ≥ 80% significantly increased from 68 to 80% between 2015 and 2020.
Most districts reported AFP cases. However, there was a decline in the NPAFP rate from 2015-2020 and few districts achieved the target rate. The suboptimal AFP surveillance system performance leaves the country at risk of missing ongoing poliovirus transmission. We recommend health worker training on active AFP searches, intensified supportive supervision, increase the number of environmental surveillance sentinel sites to boost AFP surveillance in the country, and periodic review meetings with districts to assess AFP surveillance performance.
脊髓灰质炎是由脊髓灰质炎病毒引起的疾病,可导致不可逆的瘫痪性疾病,表现为急性弛缓性麻痹(AFP)。一个敏感的 AFP 监测系统,对所有报告的 AFP 病例进行评估,首先确定它们是否为真正的 AFP 病例,是跟踪根除脊髓灰质炎的关键。真正的 AFP 病例随后被归类为脊髓灰质炎 AFP 或非脊髓灰质炎 AFP(NPAFP)病例。灵敏度的定义是满足以下标准:每年 NPAFP 率/10 万人口 < 15 岁的 ≥ 4/10 万,每年粪便充足率(SA)的 ≥ 80%。我们根据世界卫生组织推荐的指标,包括非脊髓灰质炎 AFP 和粪便充足率,描述了 2015-2020 年期间乌干达的 AFP 监测表现。
我们对 2015-2020 年期间从卫生部获得的国家 AFP 监测数据进行了描述性分析。我们评估了报告的 AFP 病例中有多少是真正的 AFP 病例,以及在研究期间 NPAFP 和粪便充足率(SA)的变化。我们评估了 2015-2020 年期间达到目标 NPAFP 和 SA 率的趋势。我们使用 QGIS 来说明各区和分区的 NPAFP 和 SA 率模式。
在 2015-2020 年期间,全国报告和调查的 3605 例 AFP 病例中,有 3475 例(96%)是真正的 AFP 病例。所有真正的 AFP 病例均与脊髓灰质炎无关。地区报告接近完成(每年 97-100%)。总体而言,NPAFP 率从 2015 年的 3.1/10 万下降到 2020 年的 2.1/10 万。不到 40%的地区在所有年份都达到了 NPAFP 目标率。达到 NPAFP 目标率的地区比例 ≥ 4/10 万显著下降,从 2015 年的 35%下降到 2020 年的 20%。全国平均年度 SA 率为 2015-2020 年的 88%。在研究期间,只有 66%的地区达到了 SA 目标率 ≥ 80%。达到 SA 率 ≥ 80%的地区比例从 2015 年的 68%显著增加到 2020 年的 80%。
大多数地区都报告了 AFP 病例。然而,从 2015 年到 2020 年,NPAFP 率下降,很少有地区达到目标率。不完善的 AFP 监测系统性能使该国面临错过正在进行的脊髓灰质炎传播的风险。我们建议对卫生工作者进行主动 AFP 搜索培训、加强支持性监督、增加环境监测哨点数量以加强该国的 AFP 监测,并定期与地区举行会议,评估 AFP 监测表现。