Zhang Wendell, Wong Lee Yung, Liu Jasmine, Sarkar Soham
University of Melbourne Clinical School, Austin Health, Heidelberg, VIC, Australia.
Emergency Department, Austin Hospital, Heidelberg, VIC, Australia.
Open Access Emerg Med. 2022 Sep 2;14:481-490. doi: 10.2147/OAEM.S376419. eCollection 2022.
Emergency Department (ED) clinicians commonly experience difficulties in referring patients to inpatient teams for hospital admission. There is limited literature reporting on patient outcomes following these complicated referrals, where ED requests for inpatient admission are rejected - which study investigators termed a "knockback".
To identify disposition outcomes and referral accuracy in ED patients whose admission referral was initially rejected. Secondary objectives were to identify additional patient, clinician and systemic factors associated with knockbacks.
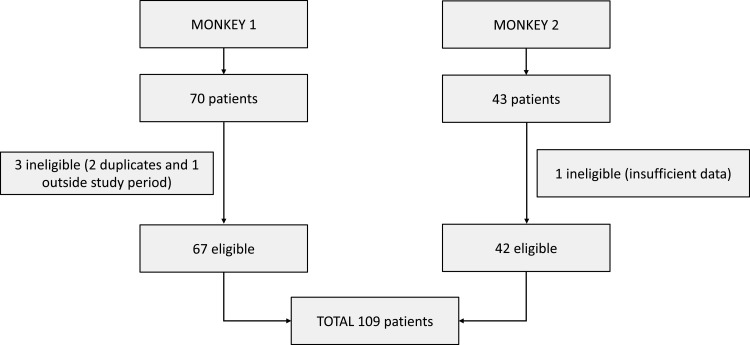
Emergency clinicians prospectively nominated a convenience sample of patients identified as having knockbacks over two time periods (Jan-Feb 2020 and Aug 2020 to Jan 2021) at a tertiary Australian ED. Data were analyzed with a mixed-methods approach and subsequent descriptive and thematic analyses were performed.
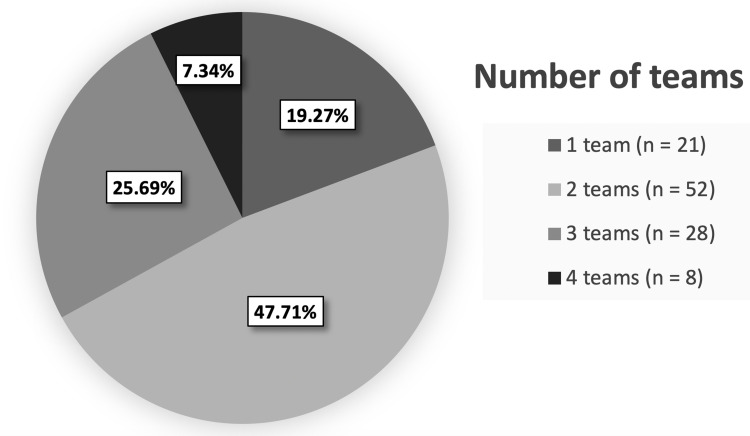
A total of 109 patients were identified as knockbacks. The referrals were warranted, with 89.0% of cases (n = 97) ultimately requiring a hospital admission. In 60.6% (n = 66) of the admissions, patients were admitted under the inpatient team initially referred to by the ED, suggesting referrals were generally accurate. The number of in-hospital units involved in the admission process and ED length of stay were positively correlated (0.409, p < 0.001). Patient factors associated with knockbacks include pre-existing chronic medical conditions and presenting acutely unwell. Analysis of clinicians' perspectives yielded recurring themes of disagreements over admission destination and diagnostic uncertainty.
In this patient sample, emergency referrals for admission were mostly warranted and accurate. Knockbacks increase ED length of stay and may adversely affect patient care. Further focused discussion and clearer referral guidelines between ED clinicians and their inpatient colleagues are required.
急诊科临床医生在将患者转介至住院团队以办理住院手续时常常遇到困难。关于这些复杂转介(即急诊科提出的住院申请被拒绝,研究人员称其为“驳回”)后患者结局的文献报道有限。
确定最初住院申请被拒绝的急诊科患者的处置结局和转介准确性。次要目标是确定与驳回相关的其他患者、临床医生和系统因素。
澳大利亚一家三级急诊科的急诊临床医生前瞻性地指定了一个便利样本,这些患者是在两个时间段(2020年1月至2月以及2020年8月至2021年1月)被确定为有申请被驳回情况的。采用混合方法对数据进行分析,并随后进行描述性和主题分析。
共确定了109例申请被驳回的患者。这些转介是合理的,89.0%的病例(n = 97)最终需要住院治疗。在60.6%(n = 66)的住院病例中,患者被最初由急诊科转介的住院团队收治,这表明转介总体上是准确的。参与住院流程的医院科室数量与急诊科住院时间呈正相关(0.409,p < 0.001)。与驳回相关的患者因素包括既往慢性病史和急性病情不佳。对临床医生观点的分析得出了关于住院目的地分歧和诊断不确定性的反复出现的主题。
在这个患者样本中,急诊住院转介大多是合理且准确的。驳回会增加急诊科住院时间,并可能对患者护理产生不利影响。急诊科临床医生与其住院同事之间需要进一步进行有针对性的讨论并制定更明确的转介指南。