James Glen, Garcia Sanchez Juan Jose, Carrero Juan Jesus, Kumar Supriya, Pecoits-Filho Roberto, Heerspink Hiddo J L, Nolan Stephen, Lam Carolyn S P, Chen Hungta, Kanda Eiichiro, Kashihara Naoki, Arnold Matthew, Kosiborod Mikhail N, Lainscak Mitja, Pollock Carol, Wheeler David C
Global Medical Affairs, BioPharmaceuticals Medical, AstraZeneca, Cambridge, UK.
Global Market Access and Pricing, BioPharmaceuticals Medical, AstraZeneca, Cambridge, UK.
Kidney Int Rep. 2022 Jun 8;7(9):2059-2070. doi: 10.1016/j.ekir.2022.05.033. eCollection 2022 Sep.
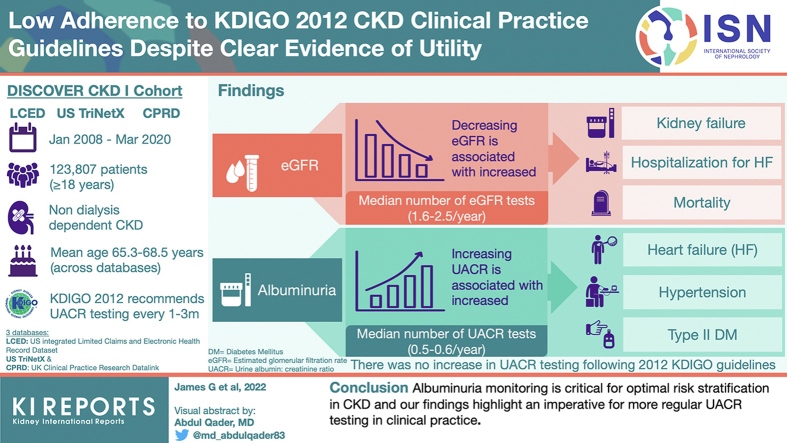
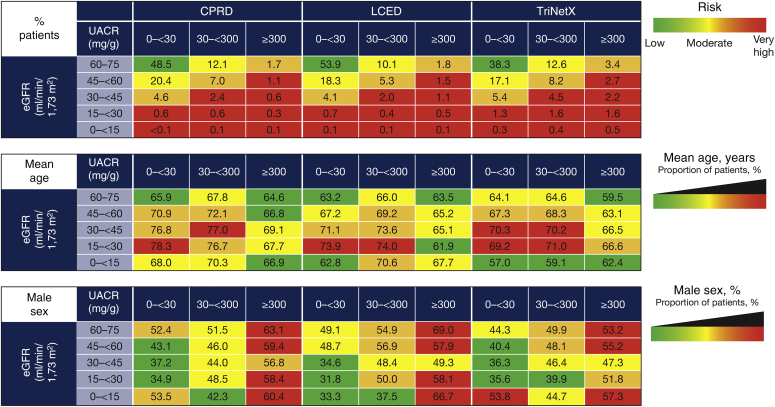
Kidney Disease: Improving Global Outcomes (KDIGO) 2012 guidelines classify chronic kidney disease (CKD) risk or prognosis using estimated glomerular filtration rate (eGFR) and urinary albumin-to-creatinine ratio (UACR). We assessed patient characteristics and outcomes according to the KDIGO classification, using data from DISCOVER CKD (NCT04034992).
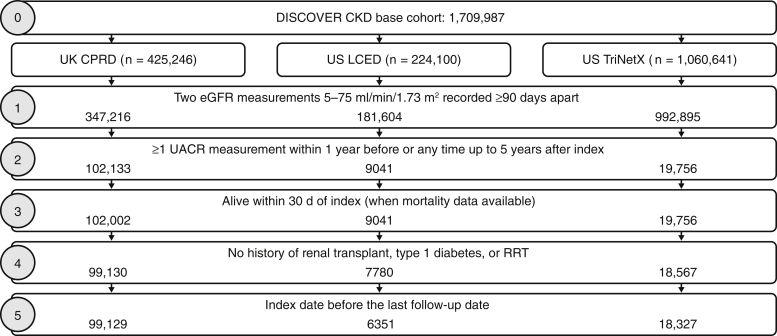
Data were extracted from the US integrated Limited Claims and Electronic Health Record Dataset and TriNetX databases, and the UK Clinical Practice Research Datalink linked to Hospital Episode Statistics and Office for National Statistics databases. Eligible patients were aged ≥18 years with CKD, and identified by 2 consecutive eGFR measures (5 to <75 ml/min/1.73 m; ≥90 days apart [maximum 730]) from January 2008. Index date was the second eGFR measurement; patients were categorized using the UACR measure closest to the index. Outcomes included patient characteristics, eGFR or UACR measurement frequency, and clinical outcomes per baseline KDIGO classification.
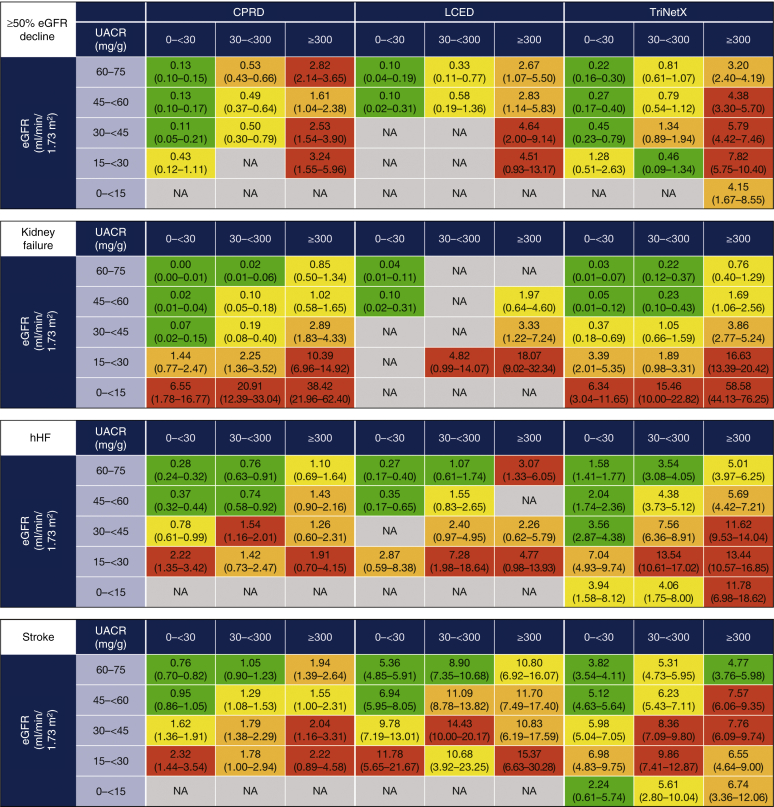
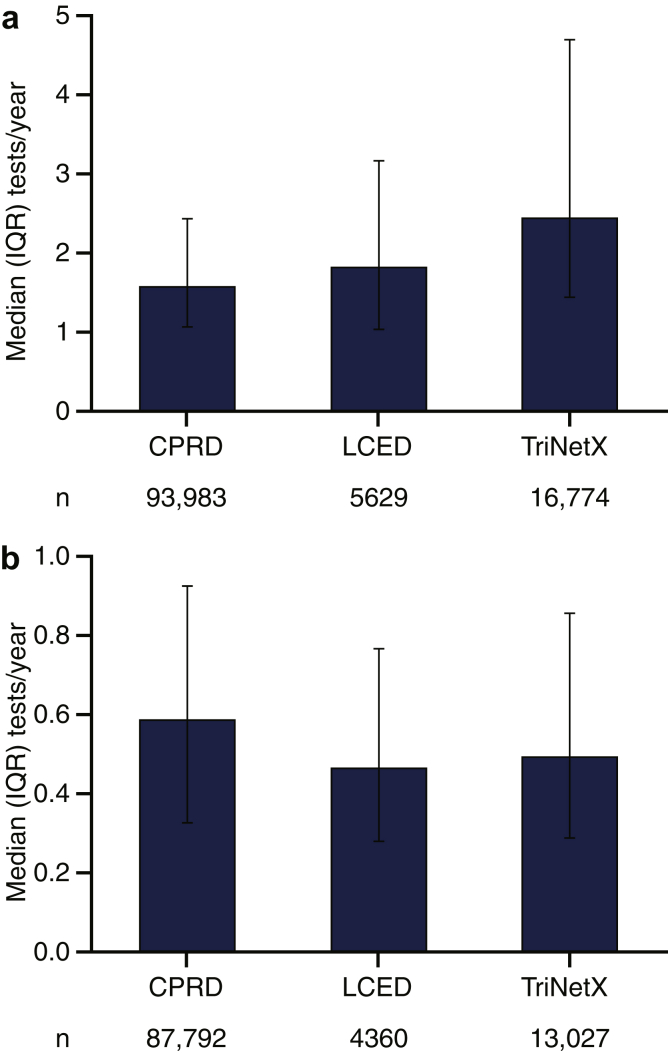
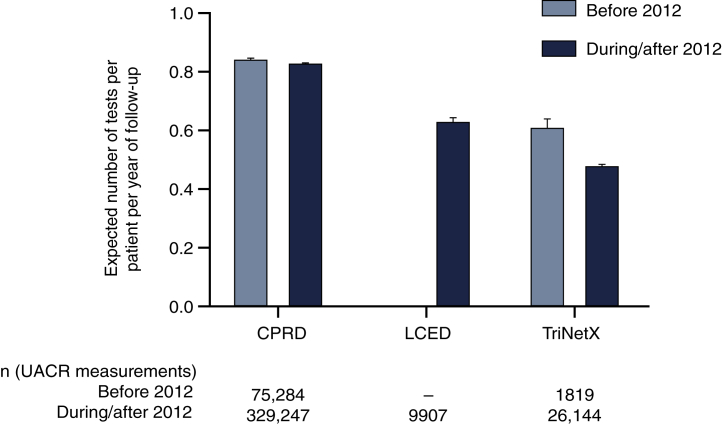
Across databases, only 8.6% of patients with 2 eGFR measures had ≥1 UACR measures. Among 123,807 eligible patients, prevalence of heart failure, hypertension, and type 2 diabetes increased with increasing albuminuria. Incidence rates of mortality and adverse cardiovascular and renal outcomes increased with declining baseline eGFR, and particularly with increasing albuminuria. Median number of eGFR and UACR tests per year post-index ranged from 1.6 to 2.5 and 0.5 to 0.6, respectively, across databases; there was no clear increase in UACR testing frequency following the KDIGO 2012 guidelines.
Albuminuria monitoring is critical for optimal risk stratification in CKD, and our findings highlight an imperative for more regular UACR testing in clinical practice.
《改善全球肾脏病预后(KDIGO)2012年指南》使用估计肾小球滤过率(eGFR)和尿白蛋白与肌酐比值(UACR)对慢性肾脏病(CKD)的风险或预后进行分类。我们利用DISCOVER CKD(NCT04034992)的数据,根据KDIGO分类评估了患者特征和预后。
数据来自美国综合有限索赔和电子健康记录数据集以及TriNetX数据库,以及与医院事件统计和国家统计局数据库相关联的英国临床实践研究数据链。符合条件的患者年龄≥18岁,患有CKD,通过2008年1月以来连续2次eGFR测量(5至<75 ml/min/1.73 m²;间隔≥90天[最长730天])确定。索引日期为第二次eGFR测量;患者根据最接近索引的UACR测量值进行分类。结局包括患者特征、eGFR或UACR测量频率以及根据基线KDIGO分类的临床结局。
在各个数据库中,仅有8.6%的接受2次eGFR测量的患者有≥1次UACR测量。在123807例符合条件的患者中,心力衰竭、高血压和2型糖尿病的患病率随蛋白尿增加而升高。死亡率以及不良心血管和肾脏结局的发生率随基线eGFR下降而升高,尤其是随着蛋白尿增加。索引后每年eGFR和UACR测试的中位数在各个数据库中分别为1.6至2.5次和0.5至0.6次;2012年KDIGO指南发布后,UACR测试频率没有明显增加。
蛋白尿监测对于CKD的最佳风险分层至关重要,我们的研究结果凸显了临床实践中更定期进行UACR测试的必要性。