van Mil Dominique, Kieneker Lyanne Marriët, Harms Evelien, Prins Grietje Harmanna, van Geer-Postmus Iris, Mepschen Maaike, Leving Marika Teresa, Stoker Nilouq, Herman Kocks Jan Willem, Gansevoort Ronald Teunis, Lambers Heerspink Hiddo Jan
Department of Clinical Pharmacy and Pharmacology, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands.
Division of Nephrology, Department of Internal Medicine, University Medical Center Groningen, University of Groningen, Groningen, the Netherlands.
EClinicalMedicine. 2025 Apr 8;82:103185. doi: 10.1016/j.eclinm.2025.103185. eCollection 2025 Apr.
Although guidelines recommend opportunistic screening for chronic kidney disease (CKD) in individuals with established risk factors, such as diabetes, hypertension, or cardiovascular disease, screening for CKD in these individuals remains suboptimal. This study aimed to evaluate the effectiveness of a systematic home-based albuminuria screening program in primary care patients at risk for CKD.
A cross-sectional screening study was performed in ten general practices and five pharmacies in the Netherlands from November 2021 to May 2024. A random selection of patients aged 45-80 years at risk for CKD based on risk factors registered in their electronic medical record was invited for home-based albuminuria screening using a urine collection device for measurement of the urinary albumin-to-creatinine ratio (ACR). In those patients with confirmed increased albuminuria (ACR ≥3 mg/mmol), an elaborate screening to assess the presence of CKD and cardiovascular risk factors was performed, followed by a referral to their general practitioner (GP) for evaluation of the findings. The primary outcome was the yield of the home-based albuminuria screening and elaborate screening to detect increased albuminuria in the GP and the pharmacy setting. SALINE is registered with ClinicalTrials.gov, NCT05321095.
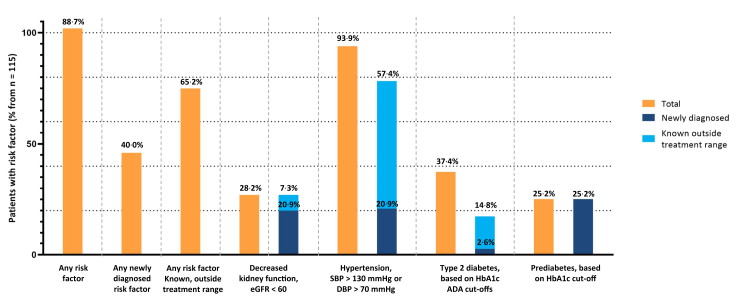
In total, 6380 patients (3802 via ten GPs and 2578 via five pharmacies) were invited for home-based albuminuria screening. The participation rate was 40·1% among patients invited via their GP (1524/3802), compared to 21·8% (562/2578) among those invited via their pharmacy (P < 0·001). In total, 8·7% of the GP participants had confirmed increased albuminuria (133/1524), compared to 6·0% of the pharmacy participants (34/562). Of the 115 GP participants with detected increased albuminuria who completed the elaborate screening, 102 (88·7%) were identified with one or more newly diagnosed CKD or cardiovascular risk factor(s) (n = 46, 40·0%), or with a known risk factor that was outside the target range for treatment (n = 75, 65·2%). Of the pharmacy participants with detected increased albuminuria completing the home-based screening, 26 completed the elaborate screening. Of those, 22 (84·6%) were identified with one or more newly diagnosed CKD or cardiovascular risk factor(s) (n = 6, 2·3%), or with a known risk factor that was outside the target range for treatment (n = 21, 80·8%).
Systematic albuminuria screening of patients at risk for CKD in primary care, when performed in addition to regular opportunistic screening, has an acceptable participation rate and yield when performed via GPs, whereas it is less effective when performed via pharmacies. Such a screening program identifies patients with yet unknown albuminuria who may benefit from starting or optimizing kidney and cardioprotective treatment. The introduction of such systematic albuminuria screening programs via GPs merits further study to optimize the participation and yield.
This study is funded by AstraZeneca Netherlands.
尽管指南建议对患有糖尿病、高血压或心血管疾病等既定风险因素的个体进行慢性肾脏病(CKD)的机会性筛查,但对这些个体进行CKD筛查的情况仍不理想。本研究旨在评估一项基于家庭的系统性蛋白尿筛查计划在有CKD风险的初级保健患者中的有效性。
2021年11月至2024年5月在荷兰的十家全科诊所和五家药店进行了一项横断面筛查研究。根据其电子病历中登记的风险因素,随机选择45 - 80岁有CKD风险的患者,邀请他们使用尿液收集装置进行家庭蛋白尿筛查,以测量尿白蛋白与肌酐比值(ACR)。对于那些确诊蛋白尿增加(ACR≥3mg/mmol)的患者,进行详细筛查以评估CKD和心血管危险因素的存在情况,然后转诊给他们的全科医生(GP)以评估检查结果。主要结局是基于家庭的蛋白尿筛查和详细筛查在全科医生诊所和药店环境中检测到蛋白尿增加的检出率。SALINE已在ClinicalTrials.gov注册,注册号为NCT05321095。
总共邀请了6380名患者(通过十家全科医生诊所邀请3802名,通过五家药店邀请2578名)进行家庭蛋白尿筛查。通过全科医生邀请的患者参与率为40.1%(1524/3802),而通过药店邀请的患者参与率为21.8%(562/2578)(P < 0.001)。通过全科医生邀请参与筛查的患者中,总共8.7%确诊蛋白尿增加(133/1524),而通过药店邀请参与筛查的患者中这一比例为6.0%(34/562)。在115名检测到蛋白尿增加且完成详细筛查的全科医生邀请参与筛查的患者中,102名(88.7%)被确定患有一种或多种新诊断的CKD或心血管危险因素(n = 46,40.0%),或患有已知的超出治疗目标范围的危险因素(n = 75,65.2%)。在检测到蛋白尿增加且完成家庭筛查的药店邀请参与筛查的患者中,26名完成了详细筛查。其中,22名(84.6%)被确定患有一种或多种新诊断的CKD或心血管危险因素(n = 6,2.3%),或患有已知的超出治疗目标范围的危险因素(n = 21,80.8%)。
在初级保健中,对有CKD风险的患者进行系统性蛋白尿筛查,若在常规机会性筛查之外进行,通过全科医生进行时参与率和检出率可接受,而通过药店进行时效果较差。这样的筛查计划可识别出蛋白尿情况未知的患者,这些患者可能从启动或优化肾脏和心脏保护治疗中获益。通过全科医生引入此类系统性蛋白尿筛查计划值得进一步研究以优化参与率和检出率。
本研究由阿斯利康荷兰公司资助。