Zou Chenchen, Wang Chentong, Lu Lin
Mudanjiang Medical College, Mudanjiang, Heilongjiang, China.
Department of Integrative Medicine-Geriatrics, Hongqi Hospital, Mudanjiang Medical College, Mudanjiang, Heilongjiang, China.
Front Physiol. 2022 Aug 24;13:960059. doi: 10.3389/fphys.2022.960059. eCollection 2022.
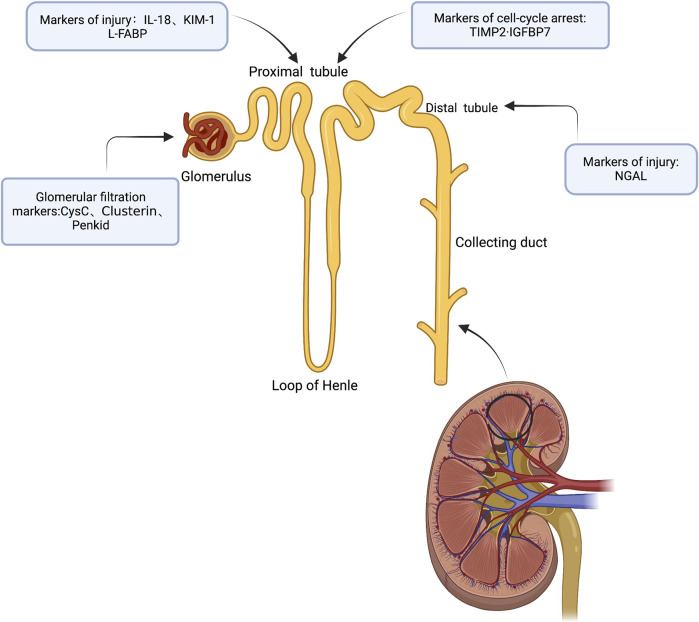
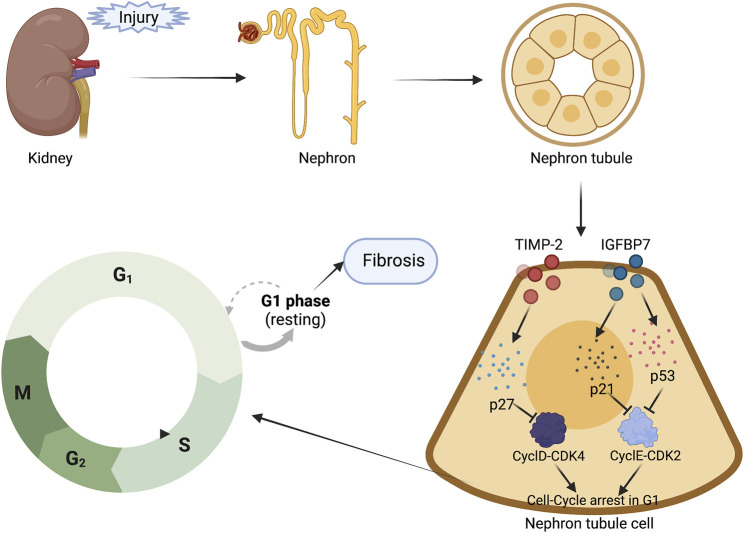
Acute kidney injury (AKI) is a prevalent and serious illness in all clinical departments, with a high morbidity and death rate, particularly in intensive care units, where prevention and treatment are crucial. As a result, active prevention, early detection, and timely intervention for acute kidney injury are critical. The current diagnostic criteria for acute kidney injury are an increase in serum creatinine concentration and/or a decrease in urine output, although creatinine and urine output merely reflect changes in kidney function, and AKI suggests injury or damage, but not necessarily dysfunction. The human kidney plays a crucial functional reserve role, and dysfunction is only visible when more than half of the renal mass is impaired. Tubular damage markers can be used to detect AKI before filtration function is lost, and new biomarkers have shown a new subset of AKI patients known as "subclinical AKI." Furthermore, creatinine and urine volume are only marginally effective for detecting subclinical AKI. As a result, the search for new biomarkers not only identifies deterioration of renal function but also allows for the early detection of structural kidney damage. Several biomarkers have been identified and validated. This study discusses some of the most promising novel biomarkers of AKI, including CysC, NGAL, KIM-1, lL-18, L-FABP, IGFBP7, TIMP-2, Clusterin, and Penkid. We examine their performance in the diagnosis of subclinical AKI, limitations, and future clinical practice directions.
急性肾损伤(AKI)在所有临床科室中都是一种普遍且严重的疾病,发病率和死亡率都很高,在重症监护病房尤其如此,在这些地方预防和治疗至关重要。因此,对急性肾损伤进行积极预防、早期检测和及时干预至关重要。目前急性肾损伤的诊断标准是血清肌酐浓度升高和/或尿量减少,尽管肌酐和尿量仅仅反映肾功能的变化,而AKI表明存在损伤,但不一定是功能障碍。人类肾脏发挥着关键的功能储备作用,只有当超过一半的肾实质受损时功能障碍才会显现出来。肾小管损伤标志物可用于在滤过功能丧失之前检测AKI,新的生物标志物已显示出一种被称为“亚临床AKI”的AKI患者新亚型。此外,肌酐和尿量对检测亚临床AKI的效果微乎其微。因此,寻找新的生物标志物不仅能识别肾功能恶化,还能实现对肾脏结构损伤的早期检测。已经鉴定并验证了几种生物标志物。本研究讨论了一些最有前景的新型AKI生物标志物,包括胱抑素C(CysC)、中性粒细胞明胶酶相关脂质运载蛋白(NGAL)、肾损伤分子-1(KIM-1)、白细胞介素-18(IL-18)、肝型脂肪酸结合蛋白(L-FABP)、胰岛素样生长因子结合蛋白7(IGFBP7)、金属蛋白酶组织抑制因子-2(TIMP-2)、簇集素(Clusterin)和肾损伤肽(Penkid)。我们研究了它们在亚临床AKI诊断中的表现、局限性以及未来临床实践方向。