Kagimu Enock, Engen Nicole, Ssebambulidde Kenneth, Kasibante John, Kiiza Tadeo K, Mpoza Edward, Tugume Lillian, Nuwagira Edwin, Nsangi Laura, Williams Darlisha A, Hullsiek Kathy Huppler, Boulware David R, Meya David B, Rhein Joshua, Abassi Mahsa, Musubire Abdu K
Infectious Diseases Institute, College of Health Sciences, Makerere University, Kampala, Uganda.
Division of Biostatistics, School of Public Health, University of Minnesota, Minneapolis, Minnesota, USA.
Open Forum Infect Dis. 2022 Aug 17;9(9):ofac416. doi: 10.1093/ofid/ofac416. eCollection 2022 Sep.
Increased intracranial pressure (ICP) frequently complicates cryptococcal meningitis. Therapeutic lumbar punctures (LPs) have acute survival benefits in the first week, and we sought to understand the longer-term survival impact of therapeutic LPs.
We prospectively enrolled human immunodeficiency virus (HIV)-seropositive adults with cryptococcal meningitis from 2013 to 2017 in Uganda. We assessed the association between clinical characteristics, CSF parameters, and 14- and 30-day mortality by baseline ICP. We also assessed 30-day mortality by number of follow-up therapeutic LPs performed within 7 days.
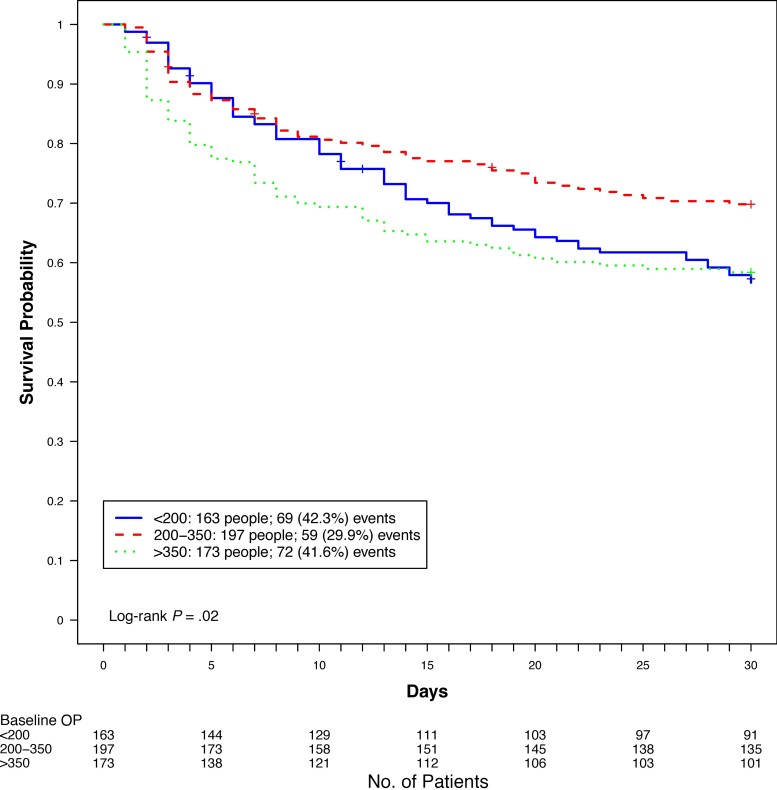
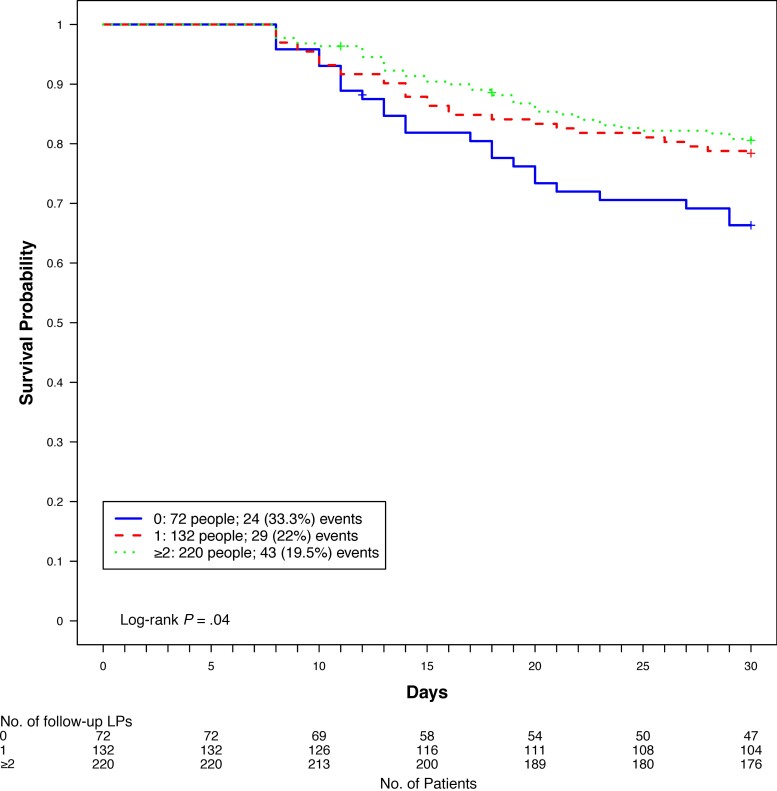
Our analysis included 533 participants. Participants with baseline ICP >350 mm HO were more likely to have Glasgow Coma Scale (GCS) score <15 ( < .001), seizures ( < .01), and higher quantitative cryptococcal cultures ( < .001), whereas participants with ICP <200 mm HO were more likely to have baseline sterile CSF cultures ( < .001) and CSF white blood cell count ≥5 cells/µL ( = .02). Thirty-day mortality was higher in participants with baseline ICP >350 mm HO and ICP <200 mm HO as compared with baseline ICP 200-350 mm HO (hazard ratio, 1.55 [95% confidence interval, 1.10-2.19]; = .02). Among survivors at least 7 days, the 30-day relative mortality was 50% higher among participants who did not receive any additional therapeutic LPs compared to those with ≥1 additional follow-up LP (33% vs 22%; = .04), irrespective of baseline ICP.
Management of increased ICP remains crucial in improving clinical outcomes in cryptococcal meningitis. Guidelines should consider an approach to therapeutic LPs that is not dictated by baseline ICP.
颅内压(ICP)升高常使隐球菌性脑膜炎病情复杂化。治疗性腰椎穿刺(LP)在第一周具有急性生存获益,我们试图了解治疗性LP对长期生存的影响。
2013年至2017年,我们在乌干达前瞻性纳入了人类免疫缺陷病毒(HIV)血清学阳性的隐球菌性脑膜炎成年患者。我们根据基线ICP评估临床特征、脑脊液参数与14天和30天死亡率之间的关联。我们还根据7天内进行的随访治疗性LP次数评估30天死亡率。
我们的分析纳入了533名参与者。基线ICP>350 mm HO的参与者更有可能出现格拉斯哥昏迷量表(GCS)评分<15(<0.001)、癫痫发作(<0.01)以及更高的隐球菌定量培养结果(<0.001),而ICP<200 mm HO的参与者更有可能出现基线脑脊液无菌培养结果(<0.001)以及脑脊液白细胞计数≥5个细胞/µL(=0.02)。与基线ICP为200 - 350 mm HO的参与者相比,基线ICP>350 mm HO和ICP<200 mm HO的参与者30天死亡率更高(风险比,1.55[95%置信区间,1.10 - 2.19];=0.02)。在至少存活7天的幸存者中,与接受≥1次额外随访LP的参与者相比,未接受任何额外治疗性LP的参与者30天相对死亡率高出50%(33%对22%;=0.04),与基线ICP无关。
控制ICP升高对于改善隐球菌性脑膜炎的临床结局仍然至关重要。指南应考虑一种不受基线ICP影响的治疗性LP方法。