Pastick Katelyn A, Bangdiwala Ananta S, Abassi Mahsa, Flynn Andrew G, Morawski Bozena M, Musubire Abdu K, Eneh Prosperity C, Schutz Charlotte, Taseera Kabanda, Rhein Joshua, Hullsiek Kathy Huppler, Nicol Melanie R, Vidal Jose E, Nakasujja Noeline, Meintjes Graeme, Muzoora Conrad, Meya David B, Boulware David R
University of Minnesota, Minneapolis, Minnesota, USA.
Infectious Diseases Institute, Makerere University, Kampala, Uganda.
Open Forum Infect Dis. 2019 Nov 5;6(11):ofz478. doi: 10.1093/ofid/ofz478. eCollection 2019 Nov.
Seizures commonly occur in patients with cryptococcal meningitis, yet risk factors and outcomes related to seizures are not well described.
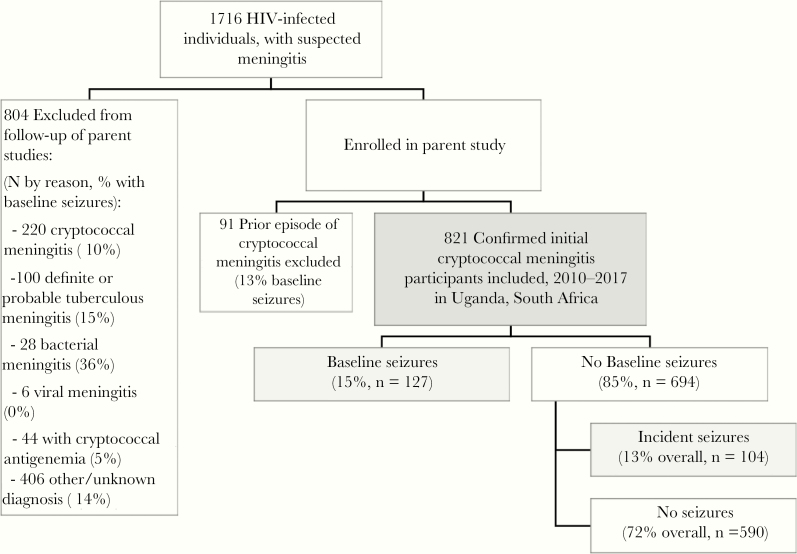
We performed post hoc analyses on participants prospectively enrolled in 3 separate human immunodeficiency virus (HIV)-associated cryptococcal meningitis clinical trials during 2010-2017. Documentation of seizures at presentation or during hospitalization and antiseizure medication receipt identified participants with seizures. We summarized participant characteristics by seizure status via Kruskal-Wallis and χ tests. Cox proportional hazards models analyzed the relationship between seizures and mortality. We compared mean quantitative neurocognitive performance Z (QNPZ-8) scores, and individual domain z-scores, at 3-months using independent tests.
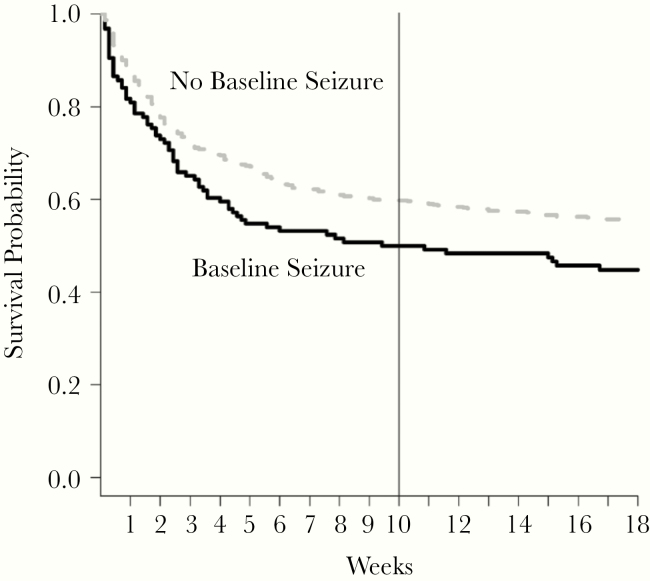
Among 821 HIV-infected cryptococcal meningitis participants, 28% (231 of 821) experienced seizures: 15.5% (127 of 821) experienced seizures at presentation, and 12.7% (104 of 821) experienced incident seizures. Participants with seizures at presentation had a significantly lower Glasgow coma scale ([GCS] <15; < .001), CD4 count (<50 cells/mcL; = .02), and higher cerebrospinal fluid (CSF) opening pressure (>25 cm HO; = .004) when compared with participants who never experienced seizures. Cerebrospinal fluid fungal burden was higher among those with seizures at presentation (125 000 colony-forming units [CFU]/mL CSF) and with seizures during follow-up (92 000 CFU/mL) compared with those who never experienced seizures (36 000 CFU/mL, < .001). Seizures were associated with increased 10-week mortality (adjusted hazard ratio = 1.45; 95% confidence interval, 1.11-1.89). Participants with seizures had lower neurocognitive function at 3 months (QNPZ-8 = -1.87) compared with those without seizures (QNPZ-8 = -1.36; < .001).
Seizures were common in this HIV-associated cryptococcal meningitis cohort and were associated with decreased survival and neurocognitive function.
癫痫发作在隐球菌性脑膜炎患者中很常见,但与癫痫发作相关的危险因素和预后情况尚未得到充分描述。
我们对2010年至2017年期间前瞻性纳入3项独立的人类免疫缺陷病毒(HIV)相关隐球菌性脑膜炎临床试验的参与者进行了事后分析。通过记录就诊时或住院期间的癫痫发作情况以及抗癫痫药物的使用情况来确定有癫痫发作的参与者。我们通过Kruskal-Wallis检验和χ²检验按癫痫发作状态总结参与者特征。Cox比例风险模型分析癫痫发作与死亡率之间的关系。我们使用独立t检验比较了3个月时的平均定量神经认知表现Z(QNPZ-8)评分以及各个领域的z评分。
在821名感染HIV的隐球菌性脑膜炎参与者中,28%(821名中的231名)经历过癫痫发作:15.5%(821名中的127名)在就诊时出现癫痫发作,12.7%(821名中的104名)出现新发癫痫发作。与从未经历过癫痫发作的参与者相比,就诊时出现癫痫发作的参与者格拉斯哥昏迷量表评分显著更低([GCS]<15;P<.001)、CD4细胞计数更低(<50个细胞/微升;P = .02),且脑脊液(CSF)初压更高(>25 cm H₂O;P = .004)。与从未经历过癫痫发作的参与者(36000菌落形成单位[CFU]/毫升脑脊液)相比,就诊时出现癫痫发作的参与者(125000 CFU/毫升脑脊液)以及随访期间出现癫痫发作的参与者(92000 CFU/毫升)的脑脊液真菌负荷更高(P<.001)。癫痫发作与10周死亡率增加相关(调整后的风险比 = 1.45;95%置信区间,1.11 - 1.89)。与未出现癫痫发作的参与者(QNPZ-8 = -1.36;P<.001)相比,出现癫痫发作的参与者在3个月时神经认知功能更低(QNPZ-8 = -1.87)。
在这个与HIV相关的隐球菌性脑膜炎队列中,癫痫发作很常见,且与生存率降低和神经认知功能下降相关。