Riad Fady S, Grau-Sepulveda Maria, Jawitz Oliver K, Vekstein Andrew M, Sundaram Varun, Sahadevan Jayakumar, Habib Robert H, Jacobs Jeffrey P, O'Brien Sean, Thourani Vinod H, Vemulapalli Sreekanth, Xian Ying, Waldo Albert L, Sabik Joseph
Harrington Heart and Vascular Institute, University Hospitals Cleveland Medical Center and Case Western Reserve University, Cleveland, Ohio.
Duke Clinical Research Institute, Durham, North Carolina.
Heart Rhythm O2. 2022 Jun 16;3(4):325-332. doi: 10.1016/j.hroo.2022.06.003. eCollection 2022 Aug.
New-onset postoperative atrial fibrillation (POAF) is the most common complication after cardiac surgery and is associated with increased long-term stroke and mortality. Anticoagulation has been suggested as a potential therapy, but data on safety and efficacy are scant.
To determine the association between anticoagulation for POAF and long-term outcomes.
Adult patients with POAF after isolated coronary artery bypass surgery (CABG) were identified through the Society of Thoracic Surgeons Adult Cardiac Surgery Database and linked to the Medicare Database. Propensity-matched analyses were performed for all-cause mortality, stroke, myocardial infarction, and major bleeding for patients discharged with or without anticoagulation. Interaction between anticoagulation and CHADS-VASc score was also assessed.
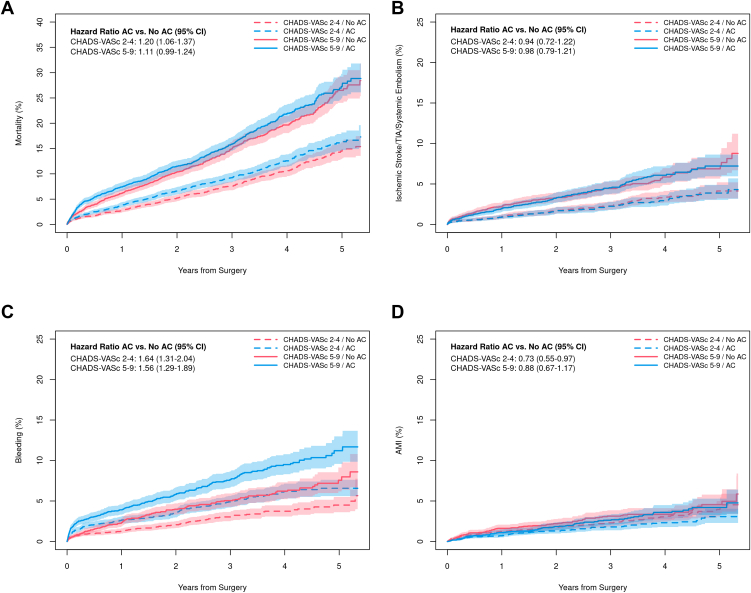
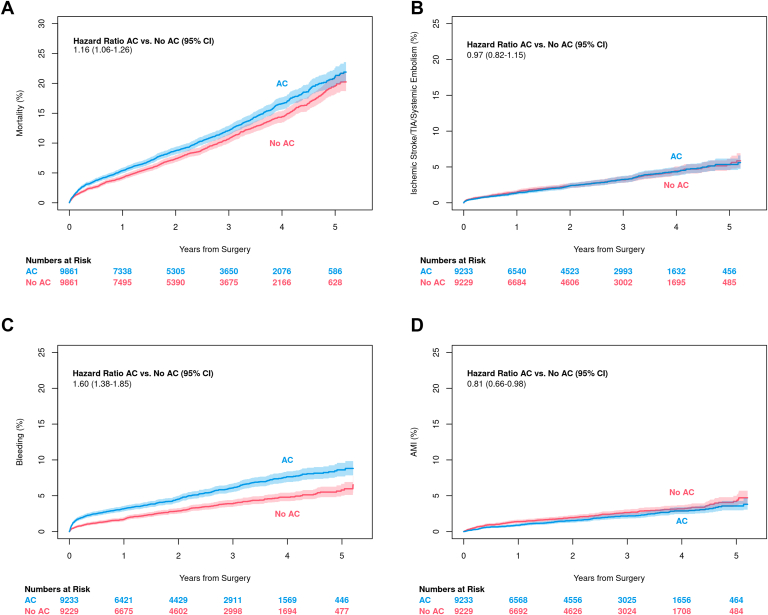
Of 38,936 patients, 9861 (25%) were discharged on oral anticoagulation. After propensity score matching, discharge anticoagulation was associated with increased mortality (hazard ratio [HR] 1.16, 95% confidence interval [CI] 1.06-1.26). There was no difference in ischemic stroke between groups (HR 0.97, 95% CI 0.82-1.15), but there was significantly higher bleeding (HR 1.60, 95% CI 1.38-1.85) among those discharged on anticoagulation. Myocardial infarction was lower in the first 30 days for those discharged on anticoagulation, but this effect decreased over time. The incidence of all complications was higher for patients with CHADS-VASc scores ≥5 compared to patients with scores of 2-4. Anticoagulation did not appear to benefit either subgroup.
Anticoagulation is associated with increased mortality after new-onset POAF following CABG. There was no reduction in ischemic stroke among those discharged on anticoagulation regardless of CHADS-VASc score.
新发术后房颤(POAF)是心脏手术后最常见的并发症,与长期中风风险增加和死亡率上升相关。抗凝治疗被认为是一种潜在的治疗方法,但关于其安全性和有效性的数据很少。
确定POAF抗凝治疗与长期预后之间的关联。
通过胸外科医师协会成人心脏手术数据库识别接受单纯冠状动脉旁路移植术(CABG)后发生POAF的成年患者,并将其与医疗保险数据库相链接。对出院时接受或未接受抗凝治疗的患者进行全因死亡率、中风、心肌梗死和大出血的倾向评分匹配分析。还评估了抗凝治疗与CHADS-VASc评分之间的相互作用。
在38936例患者中,9861例(25%)出院时接受口服抗凝治疗。倾向评分匹配后,出院时抗凝治疗与死亡率增加相关(风险比[HR]1.16,95%置信区间[CI]1.06-1.26)。两组之间缺血性中风无差异(HR 0.97,95%CI 0.82-1.15),但接受抗凝治疗出院的患者出血明显更多(HR 1.60,95%CI 1.38-1.85)。接受抗凝治疗出院的患者在术后30天内心肌梗死发生率较低,但这种效果随时间减弱。CHADS-VASc评分≥5的患者与评分为2-4的患者相比,所有并发症的发生率更高。抗凝治疗似乎对任何一个亚组都没有益处。
CABG术后新发POAF后抗凝治疗与死亡率增加相关。无论CHADS-VASc评分如何,接受抗凝治疗出院的患者缺血性中风并未减少。