Department of Gynaecologic Oncology, Division of Imaging and Oncology, University Medical Center Utrecht, Utrecht, Netherlands
Department of Gynaecologic Oncology, Division of Imaging and Oncology, University Medical Center Utrecht, Utrecht, Netherlands.
BMJ Open. 2022 Sep 13;12(9):e061829. doi: 10.1136/bmjopen-2022-061829.
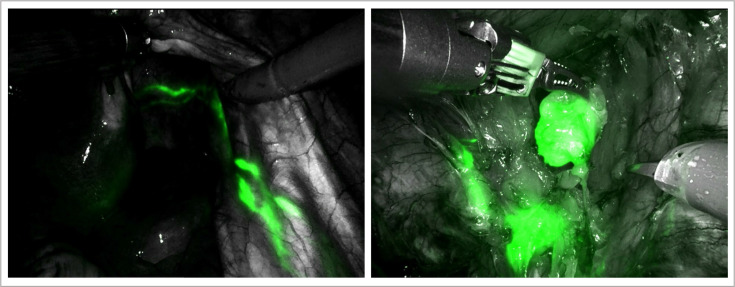
Nowadays, two predominant methods for detecting sentinel lymph nodes (SLNs) in cervical cancer are in use. The most conventional method is a combination of a radiotracer, technetium-99m (Tc) and blue dye. More recently, another method for SLN mapping using indocyanine green (ICG) is becoming widely accepted. ICG is a fluorescent dye, visualised intraoperatively with near-infrared (NIR) fluorescence imaging, providing real-time visual navigation. The presumed advantages of ICG over Tc, that is, being cheaper, non-radioactive and logistically more attractive, are only valuable if its detection rate proves to be at least non-inferior. Before omitting the well-functioning and evidence-based combined approach of Tc and blue dye, we aim to provide prospective evidence on the non-inferiority of ICG with NIR fluorescence imaging.
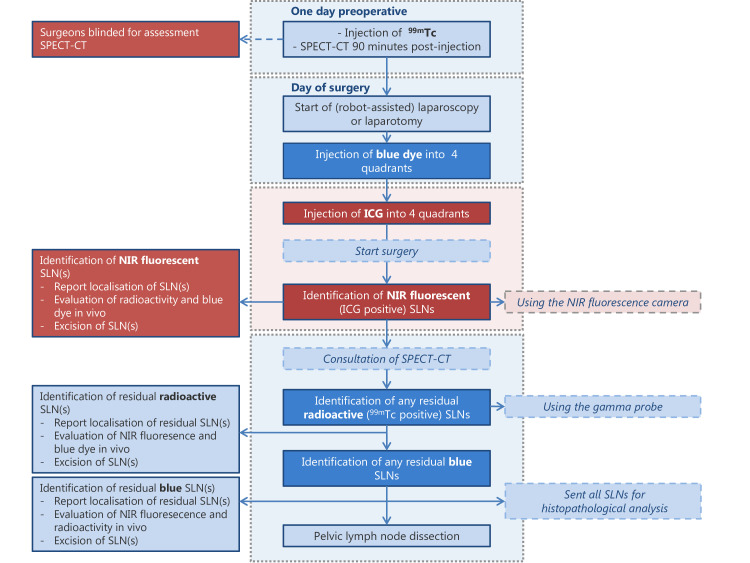
We initiated a prospective non-inferiority study with a paired comparison of both SLN methods in a single sample of 101 patients with International Federation of Gynecology and Obstetrics (FIGO) stage IA-IB2 or IIA1 cervical cancer receiving primary surgical treatment. All patients undergo SLN mapping with ICG and NIR fluorescence imaging in adjunct to mapping with Tc (including single photon emission computed tomography with X-ray computed tomography (SPECT/CT)) and blue dye. Surgeons start SLN detection with ICG while being blinded for the preoperative outcome of SPECT/CT to avoid biased detection with ICG. Primary endpoint of this study is bilateral SLN detection rate of both methods (ie, detection of at least one SLN in each hemipelvis). Since we compare strategies for SLN mapping that are already applied in current daily practice for different types of cancer, no additional risks or burdens are expected from these study procedures.
The current study is approved by the Medical Ethics Research Committee Utrecht (reference number 21-014). Findings arising from this study will be disseminated in peer-reviewed journals, academic conferences and through patient organisations.
NL9011 and EudraCT 2020-005134-15.
目前,宫颈癌前哨淋巴结(SLN)检测主要有两种方法。最常用的方法是放射性核素(锝 99mTc)联合蓝染料。最近,另一种使用吲哚菁绿(ICG)的 SLN 示踪方法也得到了广泛认可。ICG 是一种荧光染料,可通过近红外(NIR)荧光成像进行术中可视化,提供实时视觉导航。相较于锝 99mTc,ICG 的假设优势为价格更低、无放射性且在后勤方面更具吸引力,但只有当它的检测率被证明至少不劣于后者时,这些优势才具有价值。在摒弃锝 99mTc 联合蓝染料这一运作良好且有循证支持的联合方法之前,我们旨在为 ICG 联合 NIR 荧光成像的非劣效性提供前瞻性证据。
我们进行了一项前瞻性非劣效性研究,纳入了 101 例国际妇产科联合会(FIGO)分期为 IA-IB2 或 IIA1 的宫颈癌患者,所有患者均接受了原发手术治疗,采用配对比较的方法,在单个样本中比较两种 SLN 方法,即 ICG 联合 NIR 荧光成像与 Tc 联合(包括单光子发射计算机断层扫描与 X 射线计算机断层扫描[SPECT/CT])和蓝染料的 SLN 方法。所有患者均接受 ICG 和 Tc 联合 SPECT/CT 及蓝染料的 SLN 检测,术中先使用 ICG 进行 SLN 检测,同时对 SPECT/CT 的术前结果设盲,以避免 ICG 检测出现偏倚。该研究的主要终点为两种方法的双侧 SLN 检测率(即每个半骨盆中至少检测到一个 SLN)。由于我们比较的是已经应用于不同类型癌症的当前日常实践中的 SLN 映射策略,因此这些研究程序预计不会带来额外的风险或负担。
本研究已获得乌得勒支医学伦理研究委员会的批准(注册号 21-014)。该研究的结果将发表在同行评议的期刊、学术会议上,并通过患者组织进行传播。
NL9011 和 EudraCT 2020-005134-15。