Department of Cardiology, Norfolk and Norwich University Hospital, Norwich, UK.
Norwich Medical School, University of East Anglia, 2.06 Bob Champion Research and Education Building, Norwich, NR4 7TJ, UK.
Clin Res Cardiol. 2023 Sep;112(9):1186-1193. doi: 10.1007/s00392-022-02106-y. Epub 2022 Sep 14.
We aimed to investigate the safety of drug-coated balloon (DCB)-only angioplasty compared to drug-eluting stent (DES), as part of routine clinical practice.
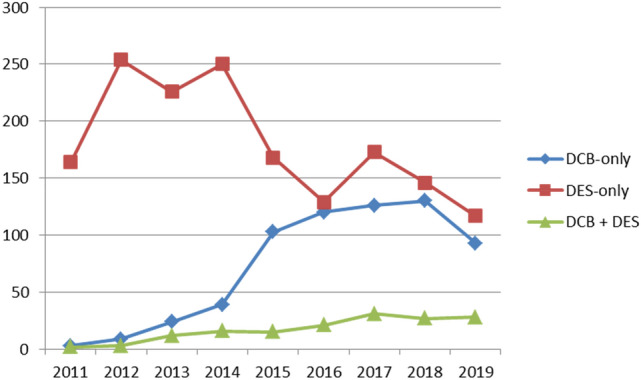
The recent BASKETSMALL2 trial demonstrated the safety and efficacy of DCB angioplasty for de novo small vessel disease. Registry data have also demonstrated that DCB angioplasty is safe; however, most of these studies are limited due to long recruitment time and a small number of patients with DCB compared to DES. Therefore, it is unclear if DCB-only strategy is safe to incorporate in routine elective clinical practice.
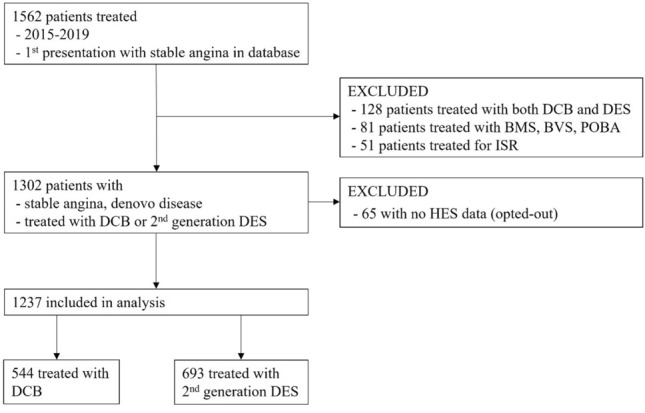
We compared all-cause mortality and major cardiovascular endpoints (MACE), including unplanned target lesion revascularisation (TLR) of all patients treated with DCB or DES for first presentation of stable angina due to de novo coronary artery disease between 1st January 2015 and 15th November 2019. Data were analysed with Cox regression models and cumulative hazard plots.
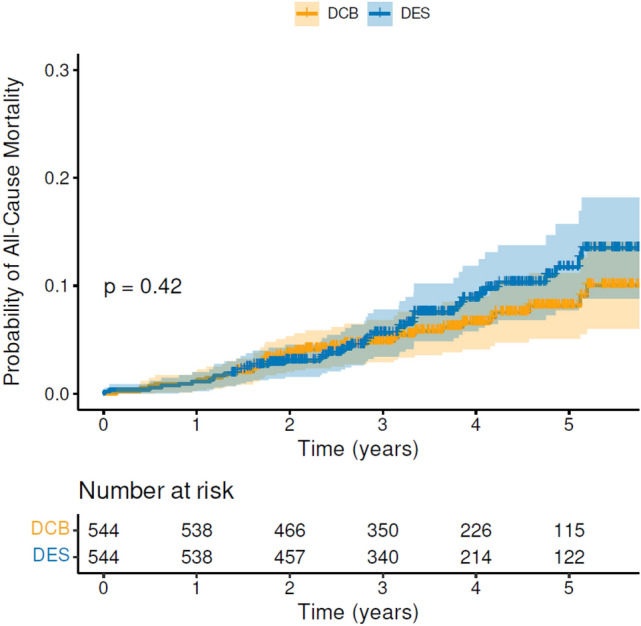
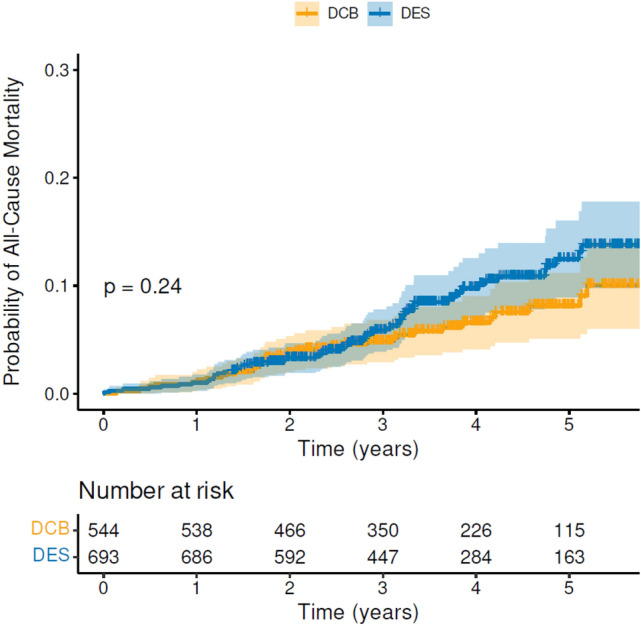
We present 1237 patients; 544 treated with DCB and 693 treated with DES for de novo, mainly large-vessel coronary artery disease. On multivariable Cox regression analysis, only age and frailty remained significant adverse predictors of all-cause mortality. Univariable, cumulative hazard plots showed no difference between DCB and DES for either all-cause mortality or any of the major cardiovascular endpoints, including unplanned TLR. The results remained unchanged following propensity score-matched analysis.
DCB-only angioplasty, for stable angina and predominantly large vessels, is safe compared to DES as part of routine clinical practice, in terms of all-cause mortality and MACE, including unplanned TLR.
我们旨在研究药物涂层球囊(DCB)血管成形术与药物洗脱支架(DES)相比的安全性,这是常规临床实践的一部分。
最近的 BASKETSMALL2 试验证明了 DCB 血管成形术治疗新发小血管疾病的安全性和有效性。注册数据还表明 DCB 血管成形术是安全的;然而,由于招募时间长,以及与 DES 相比,接受 DCB 治疗的患者数量较少,这些研究大多受到限制。因此,尚不清楚在常规择期临床实践中加入单纯 DCB 策略是否安全。
我们比较了 2015 年 1 月 1 日至 2019 年 11 月 15 日期间,因新发冠状动脉疾病首次出现稳定型心绞痛而接受 DCB 或 DES 治疗的所有患者的全因死亡率和主要心血管终点(MACE),包括计划外靶病变血运重建(TLR)。采用 Cox 回归模型和累积风险图进行数据分析。
我们纳入了 1237 例患者;544 例接受 DCB 治疗,693 例接受 DES 治疗,新发、主要为大血管冠状动脉疾病。多变量 Cox 回归分析显示,仅年龄和虚弱仍然是全因死亡率的显著不利预测因素。单变量累积风险图显示,在全因死亡率或任何主要心血管终点(包括计划外 TLR)方面,DCB 与 DES 之间无差异。倾向评分匹配分析后结果保持不变。
在常规临床实践中,对于稳定型心绞痛和主要大血管病变,与 DES 相比,单纯 DCB 血管成形术是安全的,在全因死亡率和 MACE 方面,包括计划外 TLR。