Vascularized and Composite Allotransplantation (VCA) Laboratory, Department of Plastic and Reconstructive Surgery, Johns Hopkins University School of Medicine, Baltimore, MD, United States.
Division of Nephrology, Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, United States.
Front Immunol. 2022 Sep 2;13:926648. doi: 10.3389/fimmu.2022.926648. eCollection 2022.
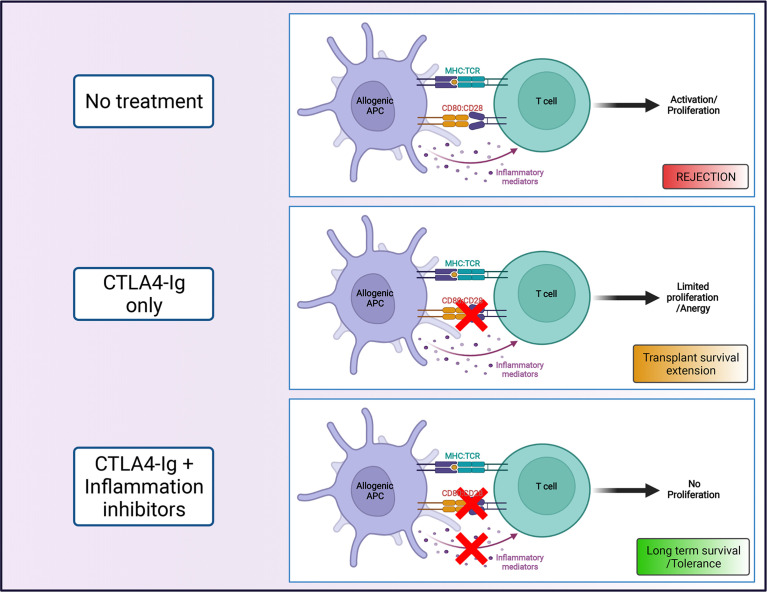
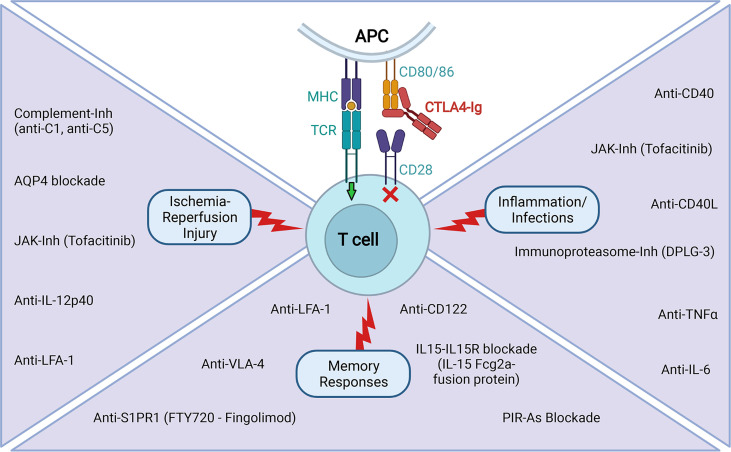
For the last few decades, Calcineurin inhibitors (CNI)-based therapy has been the pillar of immunosuppression for prevention of organ transplant rejection. However, despite exerting effective control of acute rejection in the first year post-transplant, prolonged CNI use is associated with significant side effects and is not well suited for long term allograft survival. The implementation of Costimulation Blockade (CoB) therapies, based on the interruption of T cell costimulatory signals as strategy to control allo-responses, has proven potential for better management of transplant recipients compared to CNI-based therapies. The use of the biologic cytotoxic T-lymphocyte associated protein 4 (CTLA4)-Ig is the most successful approach to date in this arena. Following evaluation of the BENEFIT trials, Belatacept, a high-affinity version of CTLA4-Ig, has been FDA approved for use in kidney transplant recipients. Despite its benefits, the use of CTLA4-Ig as a monotherapy has proved to be insufficient to induce long-term allograft acceptance in several settings. Multiple studies have demonstrated that events that induce an acute inflammatory response with the consequent release of proinflammatory cytokines, and an abundance of allograft-reactive memory cells in the recipient, can prevent the induction of or break established immunomodulation induced with CoB regimens. This review highlights advances in our understanding of the factors and mechanisms that limit CoB regimens efficacy. We also discuss recent successes in experimentally designing complementary therapies that favor CTLA4-Ig effect, affording a better control of transplant rejection and supporting their clinical applicability.
在过去的几十年中,钙调神经磷酸酶抑制剂(CNI)为基础的治疗方案一直是预防器官移植排斥反应的免疫抑制的支柱。然而,尽管在移植后第一年有效地控制了急性排斥反应,但长期使用 CNI 会引起明显的副作用,并不适合长期移植物存活。基于 T 细胞共刺激信号中断的 Costimulation Blockade(CoB)治疗策略,已被证明在控制同种反应方面具有比 CNI 为基础的治疗更好的潜力。生物制剂细胞毒性 T 淋巴细胞相关蛋白 4(CTLA4)-Ig 的使用是迄今为止该领域最成功的方法。在评估 BENEFIT 试验后,高亲和力 CTLA4-Ig 的贝那普利特已被 FDA 批准用于肾移植受者。尽管有其益处,但 CTLA4-Ig 作为单一疗法已被证明不足以在多种情况下诱导长期移植物接受。多项研究表明,在受者中引起急性炎症反应,随后释放促炎细胞因子和大量同种反应性记忆细胞的事件,可防止 CoB 方案诱导的或打破已建立的免疫调节。本综述强调了我们对限制 CoB 方案疗效的因素和机制的理解进展。我们还讨论了最近在实验设计中设计互补疗法的成功,这些疗法有利于 CTLA4-Ig 的作用,更好地控制移植排斥反应,并支持其临床适用性。