Bajaj Harnek S, Chapman Andrew W
Department of Physical Medicine and Rehabilitation, Pain Medicine, Virginia Commonwealth University Health System, Richmond, VA, USA.
Department of Anesthesiology, Chronic Pain Division, Virginia Commonwealth University Health System, Richmond, VA, USA.
Pain Rep. 2022 Sep 14;7(5):e1037. doi: 10.1097/PR9.0000000000001037. eCollection 2022 Sep-Oct.
Cervical radiofrequency neurotomy is a safe and relatively low-risk procedure commonly used to treat facet joint-mediated axial neck pain. Severe complications are extremely rare and can be avoided with proper technique and appropriate imaging guidance. This article describes the development and subsequent management of a case of dropped head syndrome after cervical radiofrequency neurotomy.
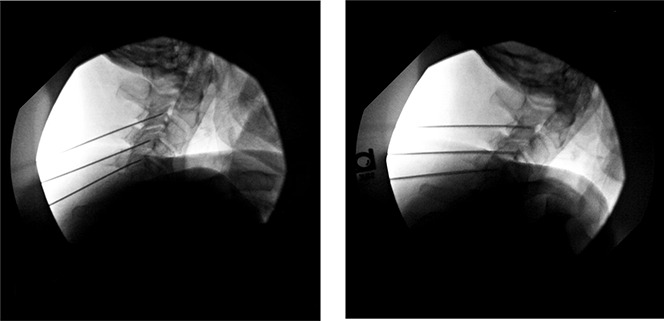
A 77-year-old man with cervicalgia, multilevel facet arthropathy, and a known kyphosis in the setting of cervical degenerative disk disease underwent successful conventional radiofrequency neurotomy to the bilateral C3, C4, and C5 medial branches. No immediate complications were noted.
Six weeks subsequent to the procedure, the patient reported difficulty keeping his head erect, and physical examination revealed weakness of the cervical paraspinal musculature, with restriction of active extension to about neutral. A diagnosis of dropped head syndrome was made. The patient was successfully managed with temporary use of soft cervical collar and physical therapy for progressive range of motion and strengthening.
Dropped head syndrome is a known, but likely underappreciated, complication of cervical radiofrequency neurotomy, with only 2 other cases reported and published in the literature to our knowledge. Mild cases may resolve with conservative management, but this is a potentially debilitating condition that we recommend should be routinely discussed during procedural consent for cervical radiofrequency neurotomy. Future studies should explore specific mitigating factors to reduce the risk of development of this possible complication.
颈椎射频神经切断术是一种安全且风险相对较低的手术,常用于治疗小关节介导的颈部轴向疼痛。严重并发症极为罕见,通过适当的技术和合适的影像引导可以避免。本文描述了一例颈椎射频神经切断术后发生低头综合征的病情发展及后续处理。
一名77岁男性,患有颈痛、多节段小关节病,且在颈椎间盘退变情况下存在已知的脊柱后凸,接受了双侧C3、C4和C5内侧支的成功常规射频神经切断术。未发现即时并发症。
术后六周,患者报告难以保持头部直立,体格检查发现颈旁脊柱肌肉无力,主动伸展受限至约中立位。诊断为低头综合征。患者通过临时使用软颈托及进行物理治疗以逐渐增加活动范围和增强肌力,得到了成功治疗。
低头综合征是颈椎射频神经切断术一种已知但可能未得到充分认识的并发症,据我们所知,文献中仅另外报道并发表了2例。轻度病例可能通过保守治疗缓解,但这是一种可能使人衰弱的病症,我们建议在颈椎射频神经切断术的手术同意过程中应常规讨论该病症。未来的研究应探索特定的减轻因素,以降低这种可能并发症发生的风险。