Department of Pharmaceutical Outcomes and Policy, College of Pharmacy, University of Florida, Gainesville, Florida, United States of America.
Center for Drug Evaluation and Safety, University of Florida, Gainesville, Florida, United States of America.
PLoS Med. 2022 Sep 22;19(9):e1004101. doi: 10.1371/journal.pmed.1004101. eCollection 2022 Sep.
Injury, prevalent and potentially associated with prescription opioid use among older adults, has been implicated as a warning sign of serious opioid-related adverse events (ORAEs) including opioid misuse, dependence, and poisoning, but this association has not been empirically tested. The study aims to examine the association between incident injury after prescription opioid initiation and subsequent risk of ORAEs and to assess whether the association differs by recency of injury among older patients.
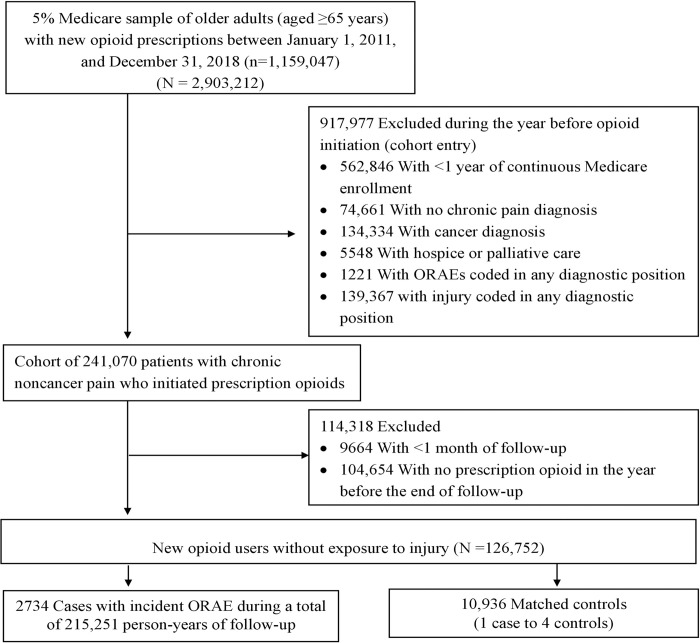
This nested case-control study was conducted within a cohort of 126,752 individuals aged 65 years or older selected from a 5% sample of Medicare beneficiaries in the United States between 2011 and 2018. Cohort participants were newly prescribed opioid users with chronic noncancer pain who had no injury or ORAEs in the year before opioid initiation, had 30 days or more of observation, and had at least 1 additional opioid prescription dispensed during follow-up. We identified ORAE cases as patients who had an inpatient or outpatient encounter with diagnosis codes for opioid misuse, dependence, or poisoning. During a mean follow-up of 1.8 years, we identified 2,734 patients who were newly diagnosed with ORAEs and 10,936 controls matched on the year of cohort entry date and a disease risk score (DRS), a summary score derived from the probability of an ORAE outcome based on covariates measured prior to cohort entry and in the absence of injury. Multivariate conditional logistic regression was used to estimate ORAE risk associated with any and recency of injury, defined based on the primary diagnosis code of inpatient and outpatient encounters. Among the cases and controls, 68.0% (n = 1,859 for cases and n = 7,436 for controls) were women and the mean (SD) age was 74.5 (6.9) years. Overall, 54.0% (n = 1,475) of cases and 46.0% (n = 1,259) of controls experienced incident injury after opioid initiation. Patients with (versus without) injury after opioid therapy had higher risk of ORAEs after adjustment for time-varying confounders, including diagnosis of tobacco or alcohol use disorder, drug use disorder, chronic pain diagnosis, mental health disorder, pain-related comorbidities, frailty index, emergency department visit, skilled nursing facility stay, anticonvulsant use, and patterns of prescription opioid use (adjusted odds ratio [aOR] = 1.4; 95% confidence interval (CI) 1.2 to 1.5; P < 0.001). Increased risk of ORAEs was associated with current (≤30 days) injury (aOR = 2.8; 95% CI 2.3 to 3.4; P < 0.001), whereas risk of ORAEs was not significantly associated with recent (31 to 90 days; aOR = 0.93; 95% CI 0.73 to 1.17; P = 0.48), past (91 to 180 days; aOR = 1.08; 95% CI 0.88 to 1.33; P = 0.51), and remote (181 to 365 days; aOR = 0.88; 95% CI 0.73 to 1.1; P = 0.18) injury preceding the incident diagnosis of ORAE or matched date. Patients with injury and prescription opioid use versus those with neither in the month before the ORAE or matched date were at greater risk of ORAEs (aOR = 5.0; 95% CI 4.1 to 6.1; P < 0.001). Major limitations are that the study findings can only be generalized to older Medicare fee-for-service beneficiaries and that unknown or unmeasured confounders have the potential to bias the observed association toward or away from the null.
In this study, we observed that incident diagnosis of injury following opioid initiation was associated with subsequent increased risk of ORAEs, and the risk was only significant among patients with injury in the month before the index date. Regular monitoring for injury may help identify older opioid users at high risk for ORAEs.
在老年人中,伤害普遍存在且可能与处方类阿片类药物的使用有关,它被认为是严重的与阿片类药物相关的不良事件(ORAEs)的警告信号,包括阿片类药物滥用、依赖和中毒,但这一关联尚未经过实证检验。本研究旨在检验处方类阿片类药物使用后发生伤害与随后发生 ORAEs 风险之间的关联,并评估在老年患者中,伤害的近期程度是否会影响这种关联。
本研究是一项嵌套病例对照研究,在 2011 年至 2018 年期间,从美国医疗保险福利计划 5%的样本中选择了 126752 名年龄在 65 岁或以上的患者作为队列人群。队列参与者是新确诊的慢性非癌痛的阿片类药物使用者,在开始使用阿片类药物前的一年中没有伤害或 ORAEs,有 30 天或更长的观察期,并且在随访期间至少有 1 次阿片类药物处方。我们将 ORAE 病例定义为在住院或门诊就诊时诊断为阿片类药物滥用、依赖或中毒的患者。在平均 1.8 年的随访期间,我们发现了 2734 例新诊断为 ORAEs 的患者和 10936 例匹配的对照者,这些对照者是基于队列进入日期和疾病风险评分(DRS)进行匹配的,DRS 是基于进入队列前和没有伤害时的合并预测 ORAE 结果的协变量计算的一个综合评分。多变量条件逻辑回归用于估计任何伤害和伤害近期程度与 ORAEs 风险之间的关联,伤害近期程度是基于住院和门诊就诊的主要诊断代码定义的。在病例和对照者中,68.0%(n=1859 例病例和 n=7436 例对照者)为女性,平均(SD)年龄为 74.5(6.9)岁。总体而言,54.0%(n=1475 例)的病例和 46.0%(n=1259 例)的对照者在开始使用阿片类药物后发生了伤害。与未发生伤害的患者相比,调整了时间相关混杂因素(包括烟草或酒精使用障碍、药物使用障碍、慢性疼痛诊断、精神健康障碍、疼痛相关合并症、衰弱指数、急诊就诊、熟练护理机构住院、抗惊厥药物使用和阿片类药物处方模式)后,发生伤害的患者发生 ORAEs 的风险更高(调整后的优势比[aOR]=1.4;95%置信区间[CI]为 1.2 至 1.5;P<0.001)。与近期(≤30 天)伤害相关的 ORAEs 风险增加(aOR=2.8;95%CI 为 2.3 至 3.4;P<0.001),而与近期(31 至 90 天;aOR=0.93;95%CI 为 0.73 至 1.17;P=0.48)、过去(91 至 180 天;aOR=1.08;95%CI 为 0.88 至 1.33;P=0.51)和长期(181 至 365 天;aOR=0.88;95%CI 为 0.73 至 1.1;P=0.18)伤害与 ORAEs 诊断或匹配日期无关。与 ORAEs 或匹配日期前的一个月既没有伤害也没有处方类阿片类药物使用的患者相比,有伤害和处方类阿片类药物使用的患者发生 ORAEs 的风险更高(aOR=5.0;95%CI 为 4.1 至 6.1;P<0.001)。主要局限性是,研究结果只能推广到老年医疗保险费用受益人群,并且未知或未测量的混杂因素有可能使观察到的关联偏向或远离零值。
在这项研究中,我们观察到阿片类药物使用后伤害的诊断与随后发生 ORAEs 的风险增加有关,并且只有在伤害发生在索引日期前一个月的患者中才具有显著意义。定期监测伤害可能有助于识别发生 ORAEs 风险较高的老年阿片类药物使用者。