Research Unit for Neurology, Odense University Hospital, Odense, Denmark; University of Southern Denmark, Odense, Denmark.
Centro Español Investigación Farmacoepidemiológica, Madrid, Spain.
JAMA Netw Open. 2022 Oct 3;5(10):e2234215. doi: 10.1001/jamanetworkopen.2022.34215.
Patients with stroke due to nontraumatic (spontaneous) intracerebral hemorrhage (ICH) often harbor vascular risk factors and comorbidities, but it is unclear which major adverse cardiovascular events (MACEs) occur more frequently among patients with a prior ICH than the general population.
To evaluate the risk of a MACE for patients with a prior ICH compared with the general population.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study identified 8991 patients with a first ICH in the Danish Stroke Registry from January 1, 2005, to June 30, 2018, who were aged 45 years or older and survived more than 30 days after an ICH. Patients in this ICH cohort were matched 1:40 on age, sex, and ICH-onset date with a comparison cohort of 359 185 individuals from the general population without a prior ICH. Both cohorts were followed up for 6 months or more until December 31, 2018, for outcomes using registry data. Data were analyzed from October 1, 2021, to July 19, 2022.
Intracerebral hemorrhage identified by a nationwide clinical database.
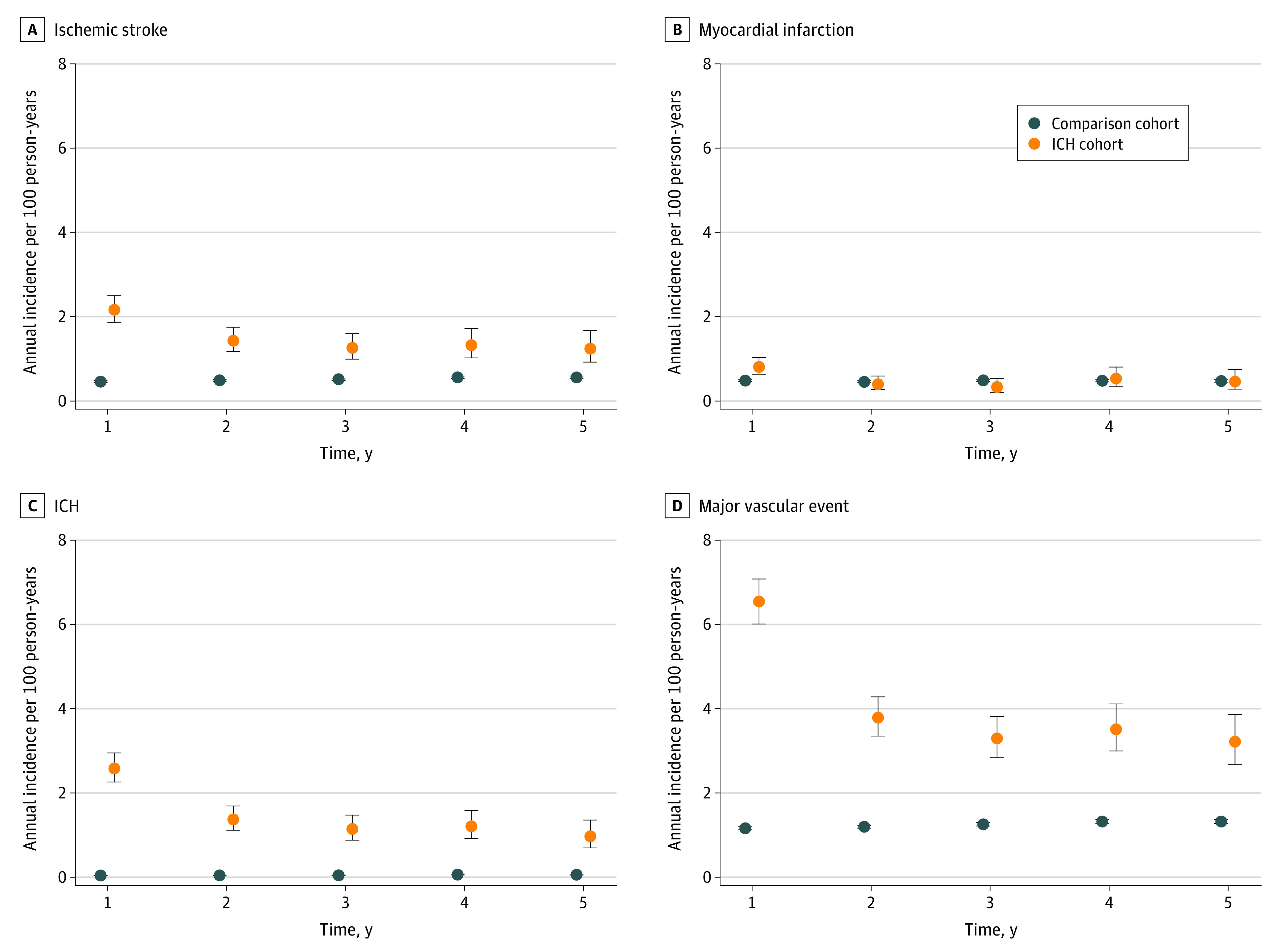
The main outcomes were ICH, ischemic stroke, myocardial infarction, and a composite of MACEs. For each outcome, a case-control study nested within the cohorts was also performed, adjusting for time-varying exposures and potential confounders. Crude absolute event rates per 100 person-years, adjusted hazard ratios (aHRs) and 95% CIs and, in the nested case-control analyses, crude and adjusted odds ratios and 95% CIs were calculated.
The ICH cohort (n = 8991; 4814 men [53.5%]; mean [SD] age, 70.7 [11.5] years) had higher event rates than the comparison cohort (n = 359 185; 192 256 men [53.5%]; mean [SD] age, 70.7 [11.5] years) for MACEs (4.16 [95% CI, 3.96-4.37] per 100 person-years vs 1.35 [95% CI, 1.33-1.36] per 100 person-years; aHR, 3.13 [95% CI, 2.97-3.30]), ischemic stroke (1.52 [95% CI, 1.40-1.65] per 100 person-years vs 0.56 [95% CI, 0.55-0.57] per 100 person-years; aHR, 2.64 [95% CI, 2.43-2.88]), and ICH (1.44 [95% CI, 1.32-1.56] per 100 person-years vs 0.06 [95% CI, 0.06-0.07] per 100 person-years; aHR, 23.49 [95% CI, 21.12-26.13]) but not myocardial infarction (0.52 [95% CI, 0.45-0.60] per 100 person-years vs 0.48 [95% CI, 0.47-0.49] per 100 person-years; aHR, 1.12 [95% CI, 0.97-1.29]). Nested case-control analyses returned risk estimates of similar magnitude as the cohort analyses.
The findings of this cohort study suggest that Danish patients with a prior ICH had statistically significantly higher rates of MACEs than the general population, indicating a need for attention to optimal secondary prevention with blood pressure lowering and antithrombotic and statin therapies after an ICH in clinical research and practice.
患有非外伤性(自发性)脑出血(ICH)的患者常伴有血管危险因素和合并症,但目前尚不清楚与一般人群相比,ICH 患者更常发生哪些主要不良心血管事件(MACE)。
评估既往有 ICH 的患者发生 MACE 的风险与一般人群相比的情况。
设计、设置和参与者:这项队列研究从 2005 年 1 月 1 日至 2018 年 6 月 30 日,在丹麦卒中登记处确定了 8991 名首次发生 ICH 的患者,这些患者年龄在 45 岁或以上,ICH 发生后存活超过 30 天。在该 ICH 队列中,年龄、性别和 ICH 发病日期与一般人群中没有 ICH 病史的 359185 人进行了 1:40 的匹配。两组患者均随访 6 个月或以上,直到 2018 年 12 月 31 日,使用登记数据进行结局评估。数据分析时间为 2021 年 10 月 1 日至 2022 年 7 月 19 日。
通过全国临床数据库识别出的脑出血。
主要结局是 ICH、缺血性卒中、心肌梗死和 MACE 复合事件。对于每个结局,还在队列内进行了病例对照研究,调整了时间变化的暴露和潜在混杂因素。每 100 人年的粗绝对事件发生率、调整后的危险比(aHR)及其 95%置信区间(CI),以及在嵌套病例对照分析中,计算了粗和调整后的比值比(OR)及其 95%CI。
ICH 队列(n=8991;4814 名男性[53.5%];平均[SD]年龄 70.7[11.5]岁)的事件发生率高于对照组(n=359185;192256 名男性[53.5%];平均[SD]年龄 70.7[11.5]岁),ICH 队列的 MACE(4.16[95%CI,3.96-4.37]/100 人年 vs 1.35[95%CI,1.33-1.36]/100 人年;aHR,3.13[95%CI,2.97-3.30])、缺血性卒中和 ICH(ICH 队列的 aHR,2.64[95%CI,2.43-2.88])发生率较高,但心肌梗死发生率较低(1.52[95%CI,1.40-1.65]/100 人年 vs 0.56[95%CI,0.55-0.57]/100 人年;0.52[95%CI,0.45-0.60]/100 人年 vs 0.48[95%CI,0.47-0.49]/100 人年;1.12[95%CI,0.97-1.29])。嵌套病例对照分析得出的风险估计与队列分析相似。
这项队列研究的结果表明,丹麦既往有 ICH 的患者发生 MACE 的风险明显高于一般人群,这表明在临床研究和实践中,需要关注在 ICH 后进行最佳的二级预防,包括降压、抗血栓和他汀类药物治疗。