Department of Medicine, University Hospitals Cleveland Medical Center, Cleveland, Ohio.
Biostatistics, Rho, Durham, North Carolina.
J Am Soc Nephrol. 2023 Jan 1;34(1):145-159. doi: 10.1681/ASN.2022040454. Epub 2022 Oct 4.
Ischemia-reperfusion (IR) of a kidney transplant (KTx) upregulates TNF α production that amplifies allograft inflammation and may negatively affect transplant outcomes.
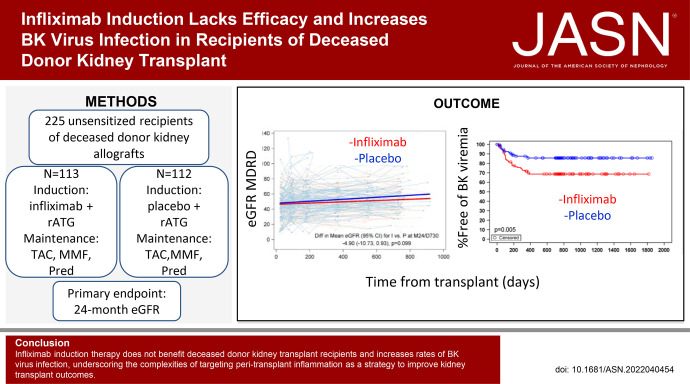
We tested the effects of blocking TNF peri-KTx via a randomized, double-blind, placebo-controlled, 15-center, phase 2 clinical trial. A total of 225 primary transplant recipients of deceased-donor kidneys (KTx; 38.2% Black/African American, 44% White) were randomized to receive intravenous infliximab (IFX) 3 mg/kg or saline placebo (PLBO) initiated before kidney reperfusion. All patients received rabbit anti-thymocyte globulin induction and maintenance immunosuppression (IS) with tacrolimus, mycophenolate mofetil, and prednisone. The primary end point was the difference between groups in mean 24-month eGFR.
There was no difference in the primary end point of 24-month eGFR between IFX (52.45 ml/min per 1.73 m 2 ; 95% CI, 48.38 to 56.52) versus PLBO (57.35 ml/min per 1.73 m 2 ; 95% CI, 53.18 to 61.52; P =0.1). There were no significant differences between groups in rates of delayed graft function, biopsy-proven acute rejection (BPAR), development of de novo donor-specific antibodies, or graft loss/death. Immunosuppression did not differ, and day 7 post-KTx plasma analyses showed approximately ten-fold lower TNF ( P <0.001) in IFX versus PLBO. BK viremia requiring IS change occurred more frequently in IFX (28.9%) versus PLBO (13.4%; P =0.004), with a strong trend toward higher rates of BKV nephropathy in IFX (13.3%) versus PLBO (4.9%; P =0.06).
IFX induction therapy does not benefit recipients of kidney transplants from deceased donors on this IS regimen. Because the intervention unexpectedly increased rates of BK virus infections, our findings underscore the complexities of targeting peritransplant inflammation as a strategy to improve KTx outcomes.Clinical Trial registry name and registration number:clinicaltrials.gov (NCT02495077).
肾移植(KTx)的缺血再灌注(IR)会上调 TNF α 的产生,从而放大移植物炎症,并可能对移植结果产生负面影响。
我们通过一项随机、双盲、安慰剂对照、225 名接受过死亡供体肾脏(KTx;38.2%为黑人/非裔美国人,44%为白人)的原发性移植患者进行了试验,这些患者被随机分配接受静脉注射英夫利昔单抗(IFX)3mg/kg 或生理盐水安慰剂(PLBO),起始于肾脏再灌注之前。所有患者均接受兔抗胸腺细胞球蛋白诱导和维持免疫抑制(IS)治疗,方案为他克莫司、霉酚酸酯和泼尼松。主要终点是两组间 24 个月时平均 eGFR 的差异。
IFX(52.45ml/min/1.73m 2 ;95%CI,48.38 至 56.52)与 PLBO(57.35ml/min/1.73m 2 ;95%CI,53.18 至 61.52;P=0.1)组间 24 个月时 eGFR 的主要终点无差异。两组在延迟移植物功能、活检证实的急性排斥反应(BPAR)、新出现的供体特异性抗体的发展、或移植物丢失/死亡方面无显著差异。免疫抑制也无差异,并且在 KTx 后第 7 天的血浆分析中,IFX 组的 TNF 水平比 PLBO 组低约十倍(P<0.001)。IFX 组(28.9%)比 PLBO 组(13.4%)更频繁地出现需要改变 IS 的 BK 病毒血症(P=0.004),IFX 组(13.3%)比 PLBO 组(4.9%)更易发生 BK 肾病(P=0.06)。
在这种 IS 方案中,IFX 诱导治疗对接受已故供体肾脏移植的患者没有益处。由于干预措施意外增加了 BK 病毒感染的发生率,我们的研究结果突显了作为改善 KTx 结果的策略,靶向移植围手术期炎症的复杂性。
clinicaltrials.gov(NCT02495077)。