Hayakawa Naoki, Takahara Mitsuyoshi, Nakama Tatsuya, Horie Kazunori, Takanashi Keisuke, Kanagami Teruaki, Ichihara Shinya, Arakawa Masataka, Tobita Kazuki, Mori Shinsuke, Iwata Yo, Suzuki Kenji, Kanda Junji
Department of Cardiovascular Medicine, Asahi General Hospital, I-1326 Asahi, Chiba, 289-2511, Japan.
Department of Metabolic Medicine, Osaka University Graduate School of Medicine, Osaka, Japan.
CVIR Endovasc. 2022 Oct 6;5(1):51. doi: 10.1186/s42155-022-00329-8.
Several studies have reported the efficacy of drug-coated balloons (DCB) for simple femoropopliteal (FP) lesions. However, the effectiveness of DCB for FP chronic total occlusive lesions (CTO) is controversial. The present study investigated the clinical outcomes of DCB for FP-CTO.
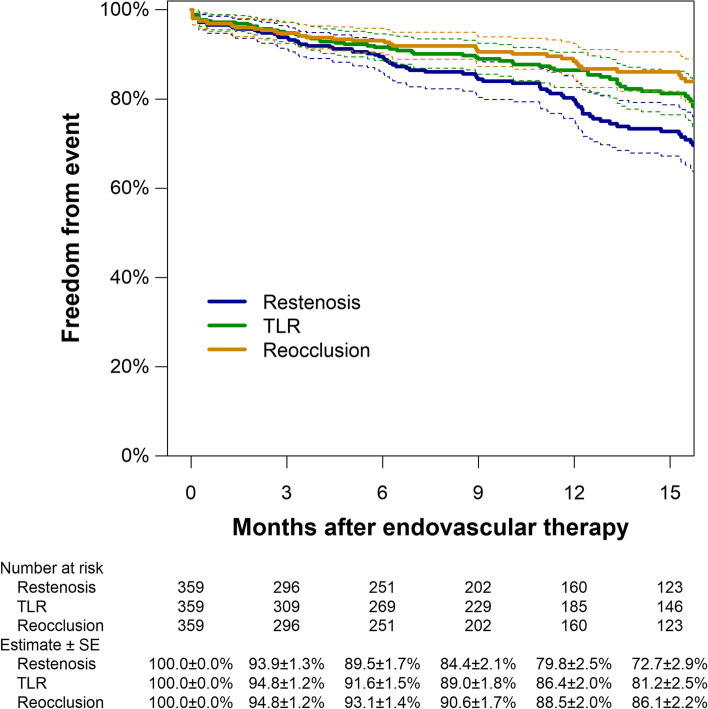
We retrospectively analyzed 359 limbs of 318 patients who underwent endovascular therapy with DCB for FP-CTO between July 2017 and February 2021 at seven cardiovascular centers. The primary endpoint was 12-month primary patency. The secondary endpoints were the 12-month rates of freedom from: (1) clinically-driven target lesion revascularization (CD-TLR), and (2) re-occlusion. The association of baseline characteristics with the 12-month restenosis risk was investigated using the Cox proportional hazards regression model.
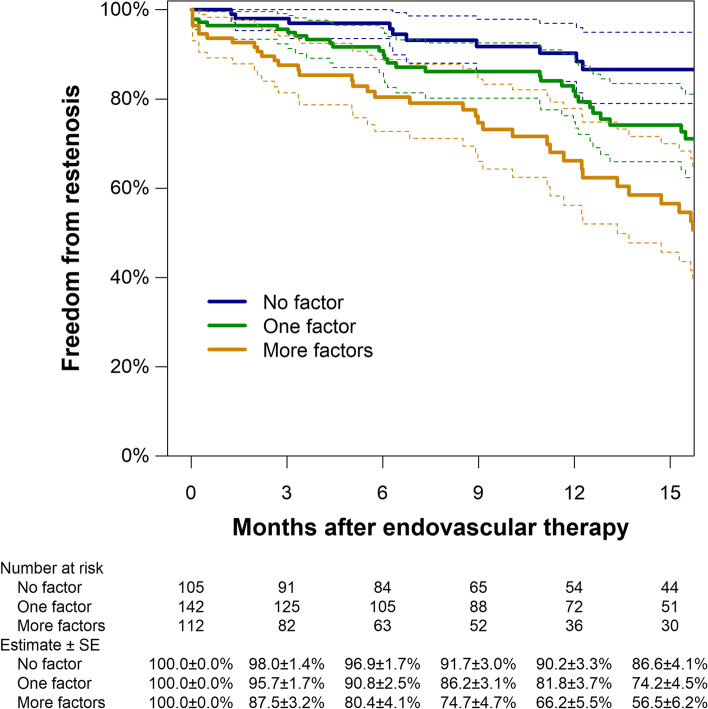
The 12-month rate of primary patency was 79.8% (95% confidence interval [95%CI], 75.1% to 84.8%), whereas the corresponding rates of freedom from CD-TLR and re-occlusion were 86.4% (95%CI: 82.6% to 90.4%) and 88.5% (95%CI: 84.7% to 92.4%), respectively. The bailout stent rate was 8.9%. Independent risk factors for restenosis were hemodialysis (adjusted hazard ratio, 2.18 [1.39 to 3.45]; P = 0.001), chronic limb-threatening ischemia (CLTI) (2.02 [1.33 to 3.07]; P = 0.001), and restenosis lesion (2.02 [1.32 to 3.08]; P = 0.001). Use of dual antiplatelet therapy (DAPT) was identified as a protective factor for restenosis (0.54 [0.35 to 0.82]; P = 0.003).
Despite the low rate of bailout stent, DCB treatment for FP-CTO was effective in real-world clinical practice. Hemodialysis, CLTI, and restenosis lesion were independent risk factors for 12-month restenosis, and the use of DAPT significantly attenuated the risk of 12-month restenosis.
多项研究报道了药物涂层球囊(DCB)治疗单纯股腘动脉(FP)病变的疗效。然而,DCB治疗FP慢性完全闭塞病变(CTO)的有效性存在争议。本研究调查了DCB治疗FP-CTO的临床结局。
我们回顾性分析了2017年7月至2021年2月期间在7个心血管中心接受DCB血管内治疗FP-CTO的318例患者的359条肢体。主要终点为12个月的原发性通畅率。次要终点为12个月的免于以下情况的发生率:(1)临床驱动的靶病变血管重建(CD-TLR),以及(2)再闭塞。使用Cox比例风险回归模型研究基线特征与12个月再狭窄风险的相关性。
12个月的原发性通畅率为79.8%(95%置信区间[95%CI],75.1%至84.8%),而相应的免于CD-TLR和再闭塞的发生率分别为86.4%(95%CI:82.6%至90.4%)和88.5%(95%CI:84.7%至92.4%)。补救性支架置入率为8.9%。再狭窄的独立危险因素为血液透析(调整后风险比,2.18[1.39至3.45];P = 0.001)、慢性肢体威胁性缺血(CLTI)(2.02[1.33至3.07];P = 0.001)和再狭窄病变(2.02[1.32至3.08];P = 0.001)。使用双联抗血小板治疗(DAPT)被确定为再狭窄的保护因素(0.54[0.35至0.82];P = 0.003)。
尽管补救性支架置入率较低,但在现实世界的临床实践中,DCB治疗FP-CTO是有效的。血液透析、CLTI和再狭窄病变是12个月再狭窄的独立危险因素,使用DAPT可显著降低12个月再狭窄的风险。