Université Paris Cité, IAME, INSERM, Paris, France.
Service de Réanimation Médicale et Infectieuse, AP-HP, Hôpital Bichat, Paris, France.
CPT Pharmacometrics Syst Pharmacol. 2022 Nov;11(11):1472-1484. doi: 10.1002/psp4.12856. Epub 2022 Oct 6.
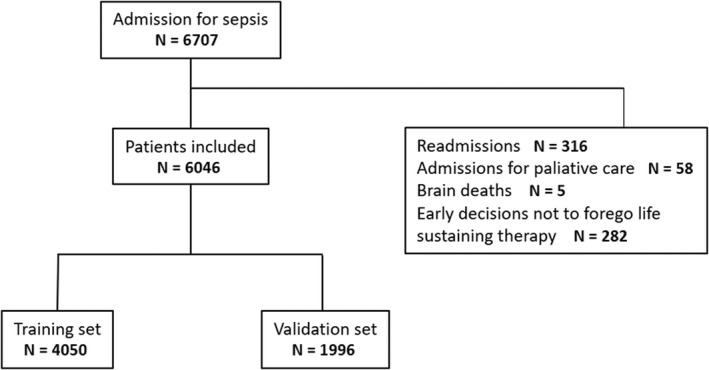
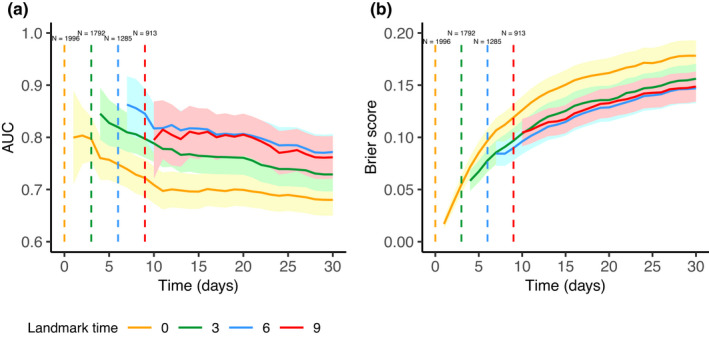
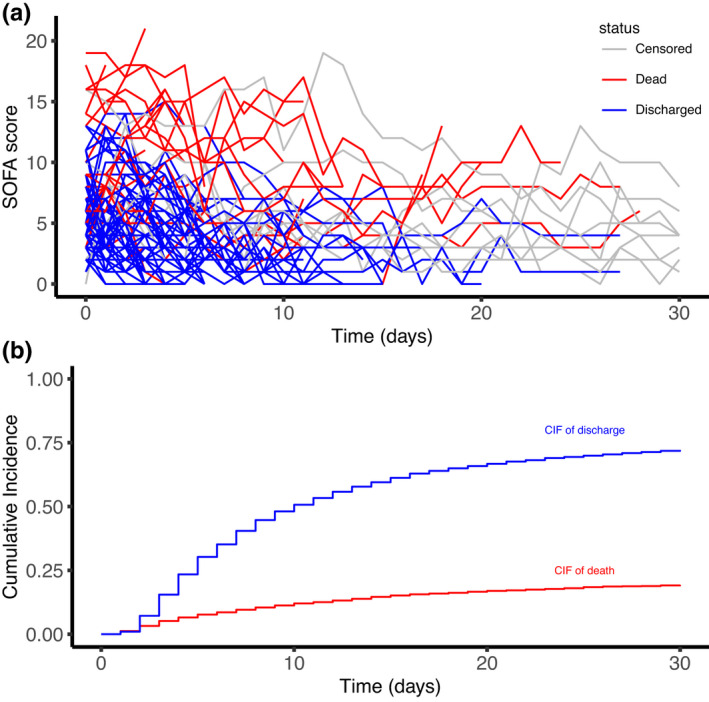
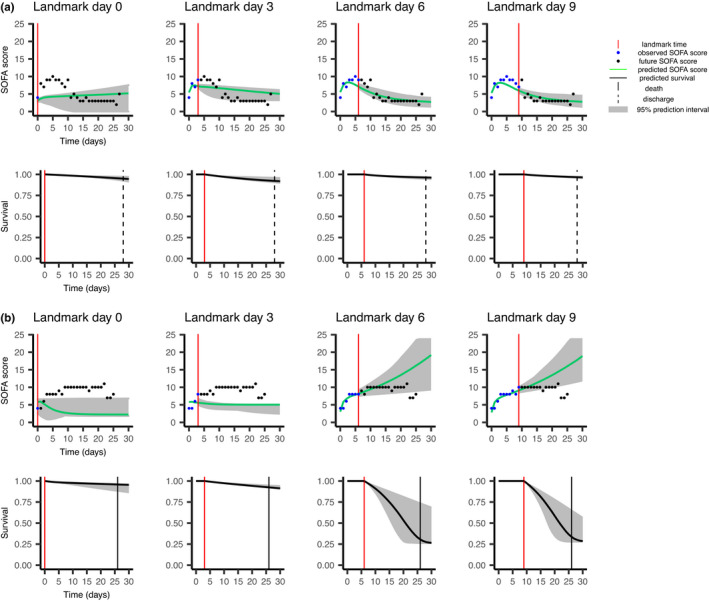
Joint models of longitudinal process and time-to-event data have recently gained attention, notably to provide individualized dynamic predictions. In the presence of competing risks, models published mostly involve cause-specific hazard functions jointly estimated with a linear or generalized linear model. Here we propose to extend the modeling to full parametric joint estimation of a nonlinear mixed-effects model and a subdistribution hazard model. We apply this approach on 6046 patients admitted in intensive care unit (ICU) for sepsis with daily Sequential Organ Failure Assessment (SOFA) score measurements. The joint model is built on a randomly selected training set of two thirds of patients and links the current predicted SOFA measurement to the instantaneous risks of ICU death and discharge from ICU, both adjusted on the patient age. Stochastic Approximation Expectation Maximization algorithm in Monolix is used for estimation. SOFA evolution is significantly associated with both risks: 0.37, 95% confidence interval (CI) = [0.35, 0.39] for the risk of death and -0.38, 95% CI = [-0.39, -0.36] for the risk of discharge. A simulation study, inspired from the real data, shows the good estimation properties of the parameters. We assess on the validation set the added value of modeling the longitudinal SOFA follow-up for the prediction of death compared with a model that includes only SOFA at baseline. Time-dependent receiver operating characteristic area under the curve and Brier scores show that when enough longitudinal individual information is available, joint modeling provides better predictions. The methodology can easily be applied to other clinical applications because of the general form of the model.
最近,纵向过程和事件时间数据的联合模型受到了关注,尤其是为了提供个体化的动态预测。在存在竞争风险的情况下,发表的模型主要涉及与线性或广义线性模型联合估计的特定原因风险函数。在这里,我们建议将建模扩展到非线性混合效应模型和亚分布风险模型的全参数联合估计。我们将这种方法应用于 6046 名因败血症入住重症监护病房(ICU)的患者,他们每天进行序贯器官衰竭评估(SOFA)评分测量。联合模型建立在三分之二的患者随机选择的训练集上,将当前预测的 SOFA 测量值与 ICU 死亡和 ICU 出院的瞬时风险联系起来,这两个风险都根据患者年龄进行了调整。Monolix 中的随机逼近期望最大化算法用于估计。SOFA 演变与这两种风险显著相关:死亡风险为 0.37,95%置信区间(CI)= [0.35, 0.39],出院风险为-0.38,95% CI = [-0.39, -0.36]。一项受真实数据启发的模拟研究表明,参数的估计性质良好。我们在验证集上评估了与仅包含基线 SOFA 的模型相比,对死亡进行预测时,对纵向 SOFA 随访进行建模的附加价值。时间依赖性接收者操作特征曲线下面积和 Brier 评分表明,当有足够的纵向个体信息时,联合建模提供了更好的预测。由于模型的通用形式,该方法可以很容易地应用于其他临床应用。