Liu Chi, Liu Xiaoli, Ma Xiaoteng, Cheng Yujing, Sun Yan, Zhang Dai, Zhao Qi, Zhou Yujie
Department of Cardiology, Beijing Anzhen Hospital, Beijing Institute of Heart Lung and Blood Vessel Disease, Beijing Key Laboratory of Precision Medicine of Coronary Atherosclerotic Disease, Clinical Center for Coronary Heart Disease, Capital Medical University, Beijing, 100029, China.
Department of Cardiology, Cardiovascular Center, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, China.
Diabetol Metab Syndr. 2022 Oct 6;14(1):145. doi: 10.1186/s13098-022-00915-9.
Measurement of estimated glucose disposal rate (eGDR) has been demonstrated to be an indicator of insulin resistance (IR) and a risk sign for long-term outcomes in those with ischemic heart disease and type 2 diabetes mellitus (T2DM) having coronary artery bypass grafting (CABG). After elective percutaneous coronary intervention (PCI), the usefulness of eGDR for prognosis in those with non-ST-segment elevation acute coronary syndrome (NSTE-ACS) and non-diabetes is yet unknown.
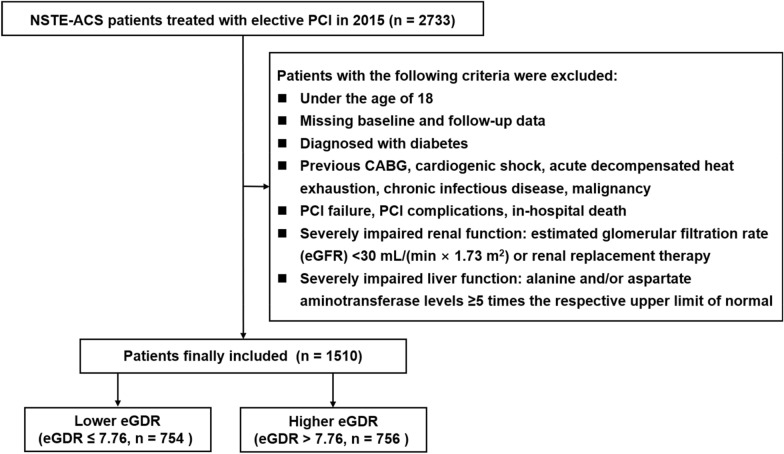
1510 NSTE-ACS patients with non-diabetes who underwent elective PCI in 2015 (Beijing Anzhen Hospital) were included in this study. Major adverse cardio-cerebral events (MACCEs), such as all-cause mortality, non-fatal myocardial infarction, non-fatal ischemic stroke, and also ischemia-driven revascularization, were the main outcome of follow-up. The average number of follow-up months was 41.84.
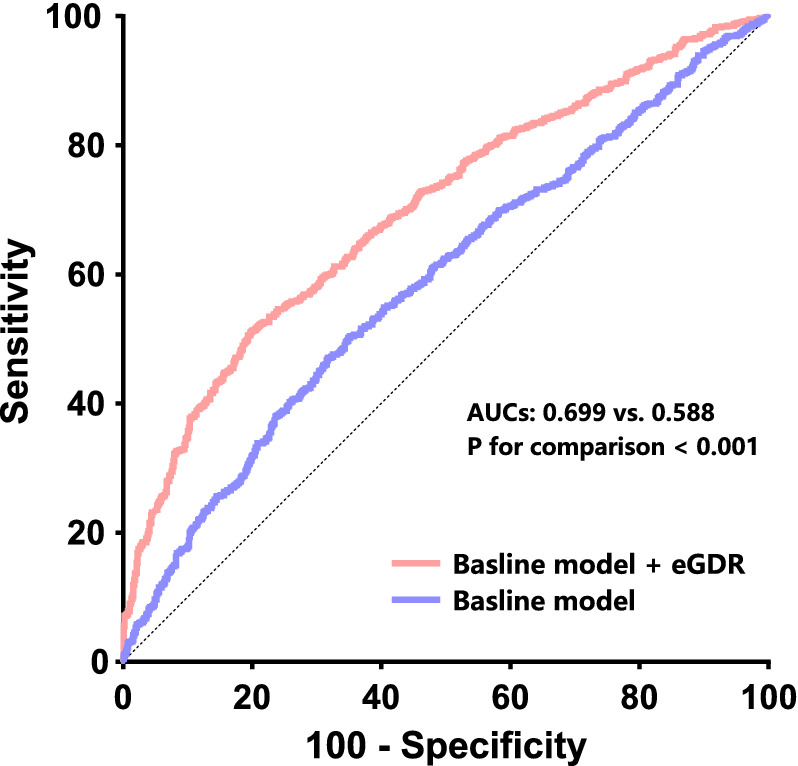
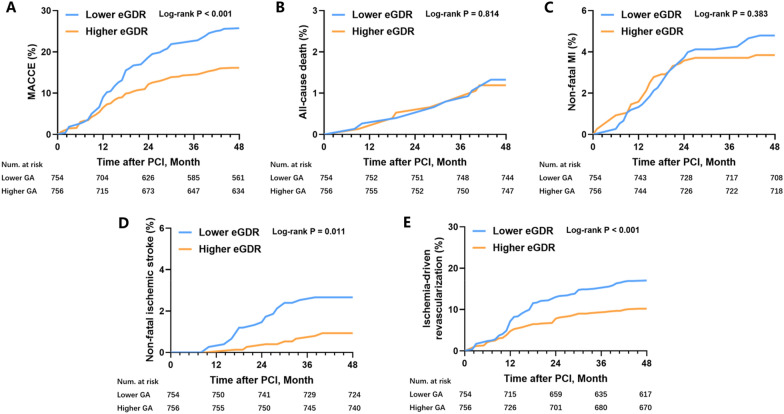
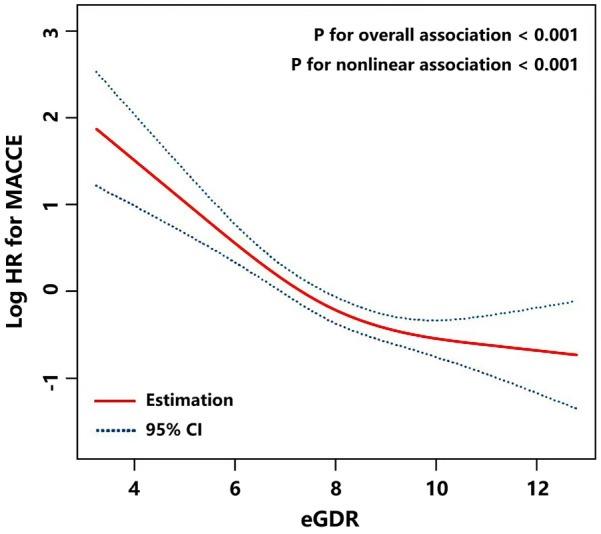
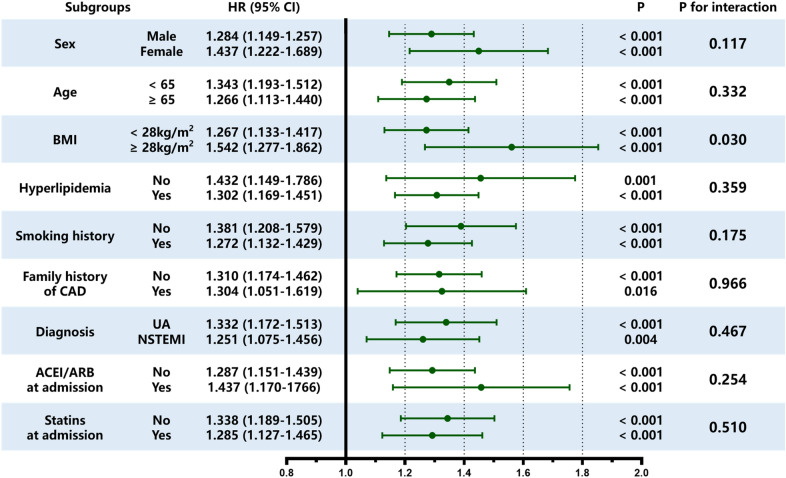
After multivariate Cox regression tests with confounder adjustment, the occurrence of MACCE in the lower eGDR cluster was considerably higher than in the higher eGDR cluster, demonstrating that eGDR is an independent prognostic indicator of MACCEs. In particular, as continuous variate: hazard ratio (HR) of 1.337, 95% confidence interval (CI) of 1.201-1.488, P < 0.001. eGDR improves the predictive power of usual cardiovascular risk factors for the primary endpoint. Specifically, the results for the area under the receiver operating characteristic (ROC) curve, this is AUC, were: baseline model + eGDR 0.699 vs. baseline model 0.588; P for contrast < 0.001; continuous net reclassification improvement (continuous-NRI) = 0.089, P < 0.001; and integrated discrimination improvement (IDI) = 0.017, P < 0.001.
Low eGDR levels showed a strong correlation with poor NSTE-ACS prognosis for nondiabetic patients undergoing PCI.
估计葡萄糖处置率(eGDR)的测量已被证明是胰岛素抵抗(IR)的指标,也是患有缺血性心脏病和2型糖尿病(T2DM)且接受冠状动脉搭桥术(CABG)患者长期预后的风险标志。在择期经皮冠状动脉介入治疗(PCI)后,eGDR对非ST段抬高型急性冠状动脉综合征(NSTE-ACS)且无糖尿病患者预后的有用性尚不清楚。
本研究纳入了2015年在北京安贞医院接受择期PCI的1510例无糖尿病的NSTE-ACS患者。主要不良心脑血管事件(MACCE),如全因死亡率、非致命性心肌梗死、非致命性缺血性卒中以及缺血驱动的血运重建,是随访的主要结局。平均随访月数为41.84。
在进行混杂因素调整的多变量Cox回归试验后,低eGDR组MACCE的发生率显著高于高eGDR组,表明eGDR是MACCE的独立预后指标。特别是,作为连续变量:风险比(HR)为1.337,95%置信区间(CI)为1.201-1.488,P < 0.001。eGDR提高了常见心血管危险因素对主要终点的预测能力。具体而言,受试者工作特征(ROC)曲线下面积(即AUC)的结果为:基线模型+eGDR为0.699,而基线模型为0.588;对比P < 0.001;连续净重新分类改善(continuous-NRI)= 0.089,P < 0.001;综合判别改善(IDI)= 0.017,P < 0.001。
低eGDR水平与接受PCI的非糖尿病患者NSTE-ACS预后不良密切相关。