Department of Thoracic Oncology, Thoraxklinik at Heidelberg University Hospital and National Center for Tumor Diseases, Heidelberg, 69126 Germany.
Institute of Pathology, Heidelberg University Hospital, Heidelberg, 69120 Germany.
Cold Spring Harb Mol Case Stud. 2022 Oct 28;8(6). doi: 10.1101/mcs.a006234. Print 2022 Oct.
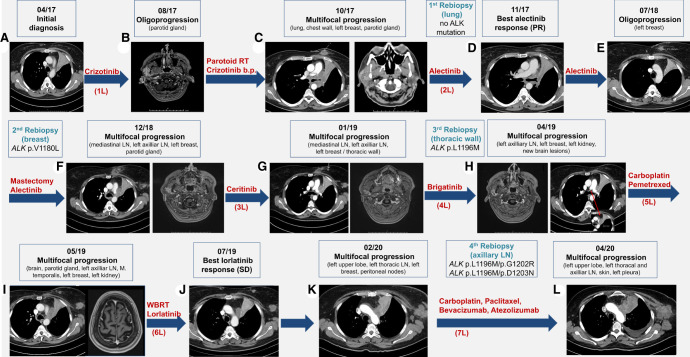
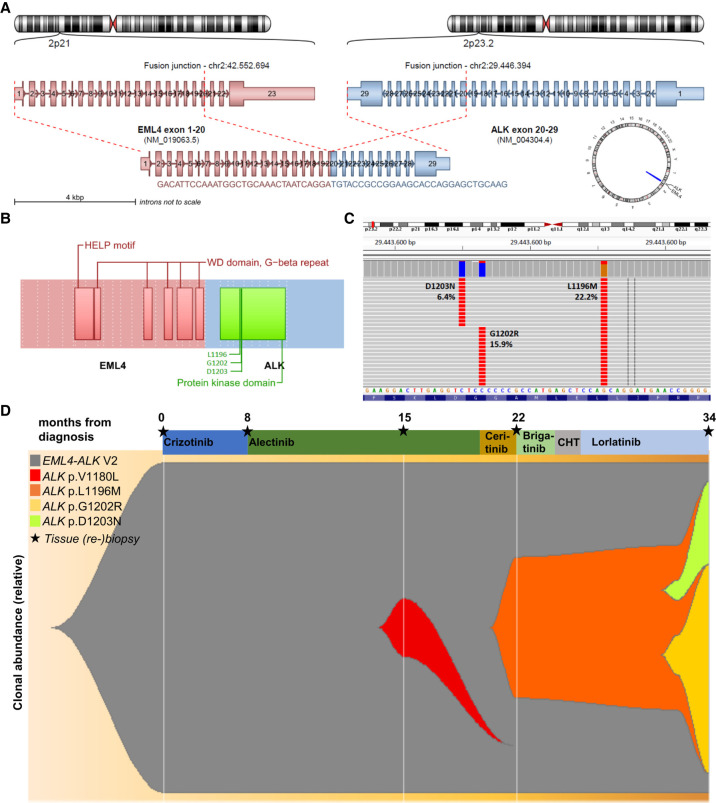
Large-cell neuroendocrine lung carcinoma (LCNEC) is a high-grade neoplasm with median survival of 1 year and limited therapeutic options. Here, we report the unusual case of a 47-yr-old female smoker with stage IV LCNEC featuring - variant 2 (E20:A20), wild-type , and low tumor mutational burden of 3.91 mut/Mb. Despite early progression within 3 mo under crizotinib, a durable response was achieved with alectinib. Oligoprogression in the left breast 10 mo later was treated by surgery, followed by a switch to ceritinib upon multifocal progression and detection of :p.V1180L in the mastectomy specimen, but without success. Another rebiopsy revealed :p.L1196M, but the tumor did not respond to brigatinib or carboplatin/pemetrexed, before stabilization under lorlatinib. Diffuse progression 8 mo later with detection of p.L1196M/p.G1202R and p.L1196M/ p.D1203N evolving from the previous p.L1196M did not respond to chemoimmunotherapy, and the patient succumbed with an overall survival (OS) of 37 mo. This case illustrates the importance of molecular profiling for LCNEC regardless of smoking status, and the superiority of next-generation ALK inhibitors compared to crizotinib for ALK+ cases. Lorlatinib retained efficacy in the heavily pretreated setting, whereas its upfront use could possibly have prevented the stepwise emergence of compound mutations. Furthermore, the disease course was more aggressive and OS shorter compared to the V2/wt ALK+ lung adenocarcinoma, whereas crizotinib, ceritinib, and brigatinib did not confer the benefit expected according to next-generation sequencing results, which also underline the need for more potent drugs against ALK in the high-risk setting of neuroendocrine histology.
大细胞神经内分泌肺癌(LCNEC)是一种高级别肿瘤,中位生存期为 1 年,治疗选择有限。在这里,我们报告了一例不寻常的 47 岁女性吸烟者,患有 IV 期 LCNEC,具有 E20:A20 变异型 2、野生型 ,肿瘤突变负担低,为 3.91 突变/Mb。尽管在克唑替尼治疗 3 个月内早期进展,但阿来替尼治疗后获得了持久的缓解。10 个月后左乳寡进展,行手术治疗,随后在多灶性进展和前次乳房切除术标本中检测到 :p.V1180L 时切换为塞瑞替尼,但无效果。再次活检显示 :p.L1196M,但肿瘤对布加替尼或卡铂/培美曲塞无反应,在洛拉替尼稳定后才稳定。8 个月后弥漫性进展,检测到 :p.L1196M/p.G1202R 和 p.L1196M/ p.D1203N 从之前的 p.L1196M 演变而来,对化疗免疫治疗无反应,患者总体生存期(OS)为 37 个月。该病例说明了无论吸烟状况如何,对 LCNEC 进行分子分析的重要性,以及下一代 ALK 抑制剂相对于克唑替尼在 ALK+病例中的优越性。洛拉替尼在预处理较多的情况下仍保持疗效,而其早期使用可能防止了复合突变的逐步出现。此外,与 V2/wt ALK+肺腺癌相比,疾病进展更具侵袭性,OS 更短,而克唑替尼、塞瑞替尼和布加替尼并未根据下一代测序结果带来预期的获益,这也强调了在神经内分泌组织学高危情况下需要更有效的针对 ALK 的药物。