Baker Heart and Diabetes Institute, Melbourne, VIC.
The Turner Institute for Brain and Mental Health, Monash University, Melbourne, VIC.
Med J Aust. 2022 Nov 21;217(10):532-537. doi: 10.5694/mja2.51734. Epub 2022 Oct 9.
To compare age-adjusted all-cause and CVD mortality, relative to the general female population, for women registered for fertility treatment who received it and those who did not.
Prospective cohort study; analysis of Monash IVF clinical registries data, 1975-2018, linked with National Death Index mortality data.
All women who registered for fertility treatment at Monash IVF (Melbourne, Victoria), 1 January 1975 - 1 January 2014, followed until 31 December 2018.
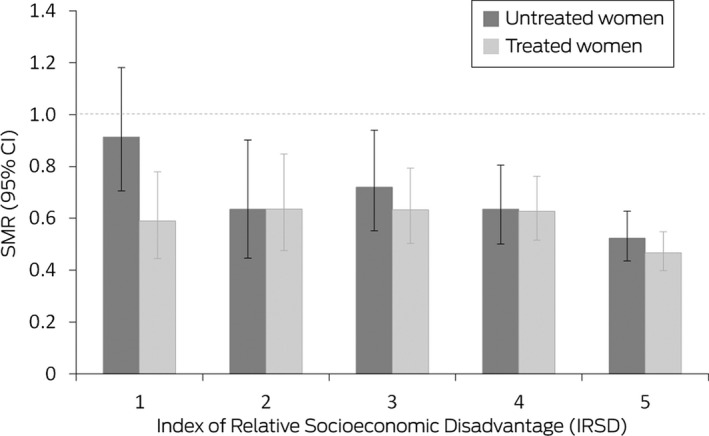
Standardised mortality ratios (SMRs) for all-cause and CVD mortality, for women who did or did not undergo fertility treatment; SMRs stratified by area-level socio-economic disadvantage (SEIFA Index of Relative Socioeconomic Disadvantage [IRSD]) and (for women who underwent treatment), by stimulated cycle number and mean oocytes/cycle categories.
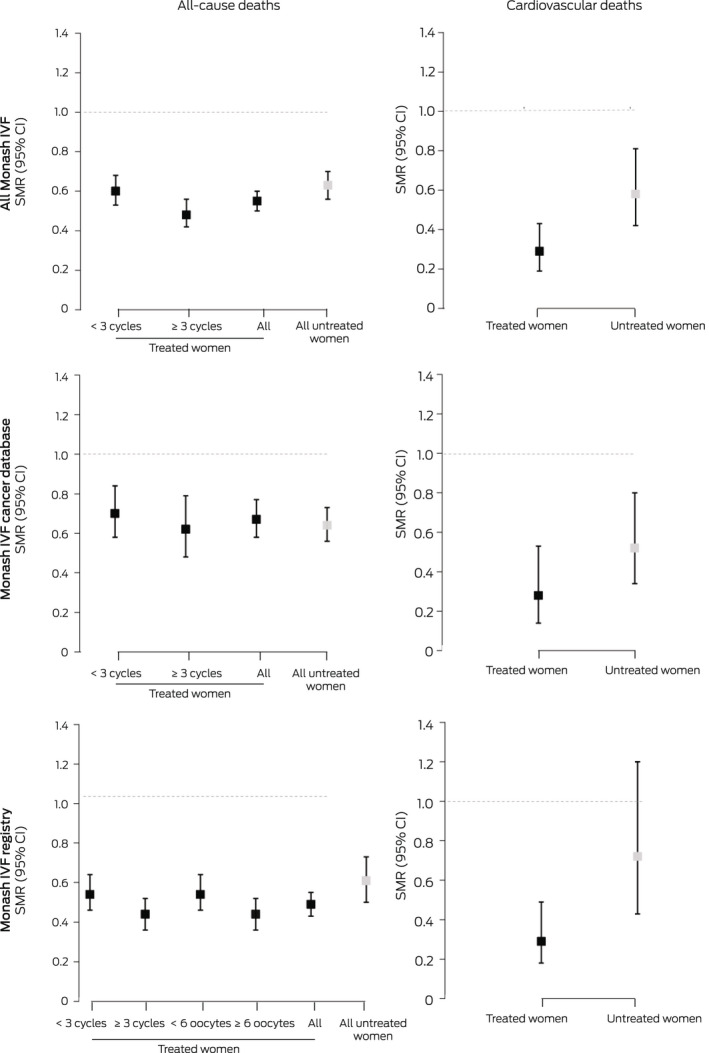
Of 44 149 women registered for fertility treatment, 33 520 underwent treatment (66.4%), 10 629 did not. After adjustment for age, both all-cause (SMR, 0.58; 95% CI, 0.54-0.62) and CVD mortality (SMR, 0.41; 95% CI, 0.32-0.53) were lower than for the general female population. All-cause mortality was similar for women registered with Monash IVF who did (SMR, 0.55; 95% CI, 0.50-0.60) or did not undergo fertility treatment (SMR, 0.63; 95% CI, 0.56-0.70). The SMR was lowest for both treated and untreated women in the fifth IRSD quintile (least disadvantage), but the difference was statistically significant only for untreated women. CVD mortality was lower for registered women who underwent fertility treatment (SMR, 0.29; 95% CI, 0.19-0.43) than for those who did not (SMR, 0.58; 95% CI, 0.42-0.81).
Fertility treatment does not increase long term all-cause or CVD mortality risk. Lower mortality among women registered for fertility treatment probably reflected their lower socio-economic disadvantage.
比较接受和未接受生育治疗的女性患者的全因和心血管疾病(CVD)死亡率,并将其与普通女性人群进行年龄校正。
前瞻性队列研究;分析莫纳什生育中心的临床注册数据,时间范围为 1975 年至 2018 年,与国家死亡指数死亡率数据相关联。
1975 年 1 月 1 日至 2014 年 1 月 1 日期间在莫纳什生育中心(维多利亚州墨尔本)登记接受生育治疗的所有女性,随访至 2018 年 12 月 31 日。
全因和 CVD 死亡率的标准化死亡率比(SMR),比较接受和未接受生育治疗的女性患者的死亡率;按地区社会经济劣势程度(SEIFA 相对社会经济劣势指数[IRSD])分层的 SMR,以及(对于接受治疗的女性)按刺激周期数和平均取卵数/周期分类的 SMR。
在 44149 名登记接受生育治疗的女性中,有 33520 名女性接受了治疗(66.4%),10629 名女性未接受治疗。在调整年龄后,全因(SMR,0.58;95%CI,0.54-0.62)和 CVD 死亡率(SMR,0.41;95%CI,0.32-0.53)均低于普通女性人群。在莫纳什生育中心登记的女性中,接受生育治疗(SMR,0.55;95%CI,0.50-0.60)或未接受生育治疗(SMR,0.63;95%CI,0.56-0.70)的全因死亡率相似。在社会经济劣势程度最低的第五个 IRSD 五分位数中,接受和未接受治疗的女性的 SMR 均最低,但仅未接受治疗的女性的差异具有统计学意义。接受生育治疗的女性的 CVD 死亡率低于未接受治疗的女性(SMR,0.29;95%CI,0.19-0.43)(SMR,0.58;95%CI,0.42-0.81)。
生育治疗不会增加长期全因或 CVD 死亡率风险。接受生育治疗的女性死亡率较低可能反映了她们较低的社会经济劣势程度。