Zhao Xin, Liu Jian-Feng, Su Xin, Long De-Yong, Sang Cai-Hua, Tang Ri-Bo, Yu Rong-Hui, Liu Nian, Jiang Chen-Xi, Li Song-Nan, Guo Xue-Yuan, Wang Wei, Zuo Song, Dong Jian-Zeng, Ma Chang-Sheng
Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, China.
Department of Cardiology, The Second Medical Center and National Clinical Research Center for Geriatric Diseases, Chinese People's Liberation Army General Hospital, Beijing, China.
Front Cardiovasc Med. 2022 Sep 23;9:984251. doi: 10.3389/fcvm.2022.984251. eCollection 2022.
Acute pericardial tamponade (APT) is one of the most serious complications of catheter ablation for atrial fibrillation (AF-CA). Direct autotransfusion (DAT) is a method of reinjecting pericardial blood directly into patients through vein access without a cell-salvage system. Data regarding DAT for APT are rare and provide limited information. Our present study aims to further investigate the safety and feasibility of DAT in the management of APT during the AF-CA procedure.
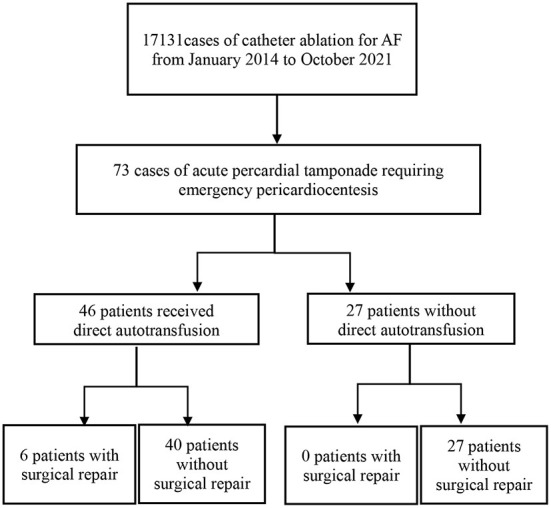
We retrospectively reviewed 73 cases of APT in the perioperative period of AF-CA from January 2014 to October 2021 at our institution, among whom 46 were treated with DAT. All included patients successfully received emergency pericardiocentesis through subxiphoid access guided by X-ray. Larger volumes of aspirated pericardial blood (658.4 ± 545.2 vs. 521.2 ± 464.9 ml), higher rates of bridging anticoagulation (67.4 vs. 37.0%), and surgical repair (6 vs. 0) were observed in patients with DAT than without. Moreover, patients with DAT were less likely to complete AF-CA procedures (32/46 vs. 25/27) and had a lower incidence of APT first presented in the ward (delayed presentation) (8/46 vs. 9/27). There was no difference in major adverse events (death/disseminated intravascular coagulation/multiple organ dysfunction syndrome and clinical thrombosis) (0/0/1/0 vs. 1/0/0/0), other potential DAT-related complications (fever/infection and deep venous thrombosis) (8/5/2 vs. 5/3/1), and length of hospital stay (11.4 ± 11.6 vs. 8.3 ± 4.7 d) between two groups.
DAT could be a feasible and safe method to deal with APT during AF-CA procedure.
急性心包填塞(APT)是心房颤动导管消融术(AF-CA)最严重的并发症之一。直接自体输血(DAT)是一种在没有细胞回收系统的情况下,通过静脉通路将心包积血直接回输给患者的方法。关于DAT治疗APT的数据很少,提供的信息有限。我们目前的研究旨在进一步探讨DAT在AF-CA手术中治疗APT的安全性和可行性。
我们回顾性分析了2014年1月至2021年10月在我院AF-CA围手术期发生APT的73例患者,其中46例接受了DAT治疗。所有纳入患者均在X线引导下经剑突下入路成功接受了紧急心包穿刺术。与未接受DAT治疗的患者相比,接受DAT治疗的患者吸出的心包积血体积更大(658.4±545.2 vs. 521.2±464.9 ml),桥接抗凝率更高(67.4% vs. 37.0%),手术修复率更高(6例 vs. 0例)。此外,接受DAT治疗的患者完成AF-CA手术的可能性较小(32/46 vs. 25/27),且在病房首次出现APT(延迟表现)的发生率较低(8/46 vs. 9/27)。两组在主要不良事件(死亡/弥散性血管内凝血/多器官功能障碍综合征和临床血栓形成)(0/0/1/0 vs. 1/0/0/0)、其他潜在的与DAT相关的并发症(发热/感染和深静脉血栓形成)(8/5/2 vs. 5/3/1)以及住院时间(11.4±11.6 vs. 8.3±4.7天)方面无差异。
DAT可能是AF-CA手术中处理APT的一种可行且安全的方法。