Wang He, Liu Tingting, Chen Jun, Dang Jun
Department of Radiation Oncology, The First Hospital of China Medical University, Shenyang, China.
Department of Radiation Oncology, Anshan Cancer Hospital, Anshan, China.
Front Oncol. 2022 Sep 21;12:901494. doi: 10.3389/fonc.2022.901494. eCollection 2022.
It remains uncertain whether neoadjuvant immune checkpoint inhibitor (nICI) is superior to neoadjuvant chemotherapy (nCT) in resectable non-small cell lung cancer. In addition, there are outstanding questions for nICI such as the ideal treatment mode and predictors.
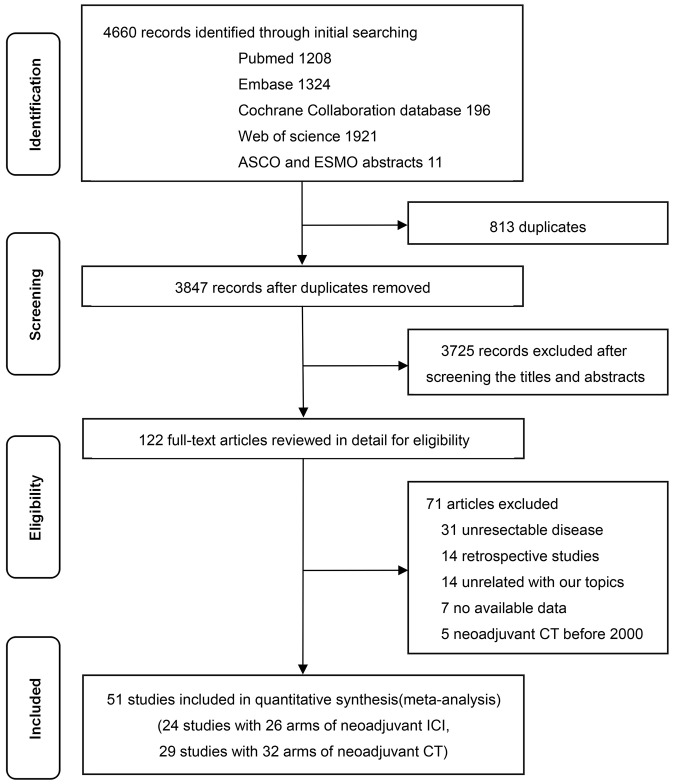
PubMed, Embase, Cochrane Library, Web of Science, and scientific meetings were searched for eligible single-arm or multi-arm trials until 31 December 2021. The primary outcomes of interest were major pathological response (MPR) and pathological complete response (pCR). The random-effect model was used for statistical analysis.
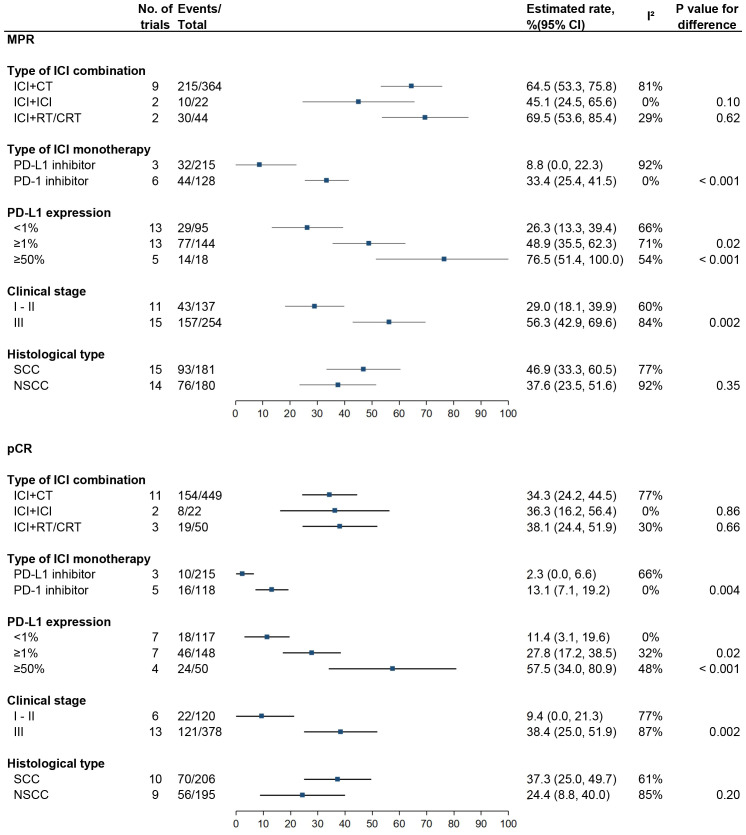
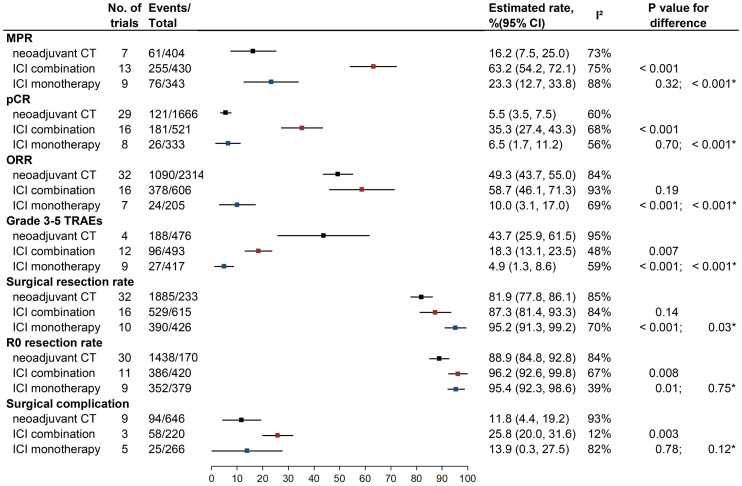
Twenty-four trials of nICI (n = 1,043) and 29 trials of nCT (n = 2,337) were identified. nICI combination therapy was associated with higher MPR (63.2%, 95% CI: 54.2%-72.1%) and pCR (35.3%, 95% CI: 27.4%-43.3%) rates compared to nCT (16.2%, 95% CI: 7.5%-25.0%, P < 0.001 and 5.5%, 95% CI: 3.5%-7.5%, P < 0.001) and nICI monotherapy (23.3%, 95% CI: 12.7%-33.8%, P < 0.001, and 6.5%, 95% CI: 1.7%-11.2%, P < 0.001). As for safety, nICI monotherapy had the best tolerability; nICI combination showed a similar surgical resection rate and higher R0 resection rate compared to nCT. PD-1 inhibitor and high PD-L1 expression (≥1% or ≥50%) were correlated with higher MPR and pCR rates compared to PD-L1 inhibitor and PD-L1 expression <1%.
nICI combination therapy is associated with higher MPR and pCR rates compared to nCT and nICI monotherapy. PD-1 inhibitor seems to be superior to PD-L1 inhibitor. PD-L1 status appears to be predictive of MPR and pCR for patients receiving nICI.
https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=278661, CRD42021278661.
在可切除的非小细胞肺癌中,新辅助免疫检查点抑制剂(nICI)是否优于新辅助化疗(nCT)仍不确定。此外,nICI还存在一些突出问题,如理想的治疗模式和预测指标。
检索了PubMed、Embase、Cochrane图书馆、Web of Science以及科学会议,以查找截至2021年12月31日符合条件的单臂或多臂试验。主要关注的结局是主要病理缓解(MPR)和病理完全缓解(pCR)。采用随机效应模型进行统计分析。
共纳入24项nICI试验(n = 1,043)和29项nCT试验(n = 2,337)。与nCT(16.2%,95%CI:7.5%-25.0%,P < 0.001)和nICI单药治疗(23.3%,95%CI:12.7%-33.8%,P < 0.001)相比,nICI联合治疗的MPR(63.2%,95%CI:54.2%-72.1%)和pCR(35.3%,95%CI:27.4%-43.3%)率更高。在安全性方面,nICI单药治疗的耐受性最佳;与nCT相比,nICI联合治疗的手术切除率相似,但R0切除率更高。与PD-L1抑制剂和PD-L1表达<1%相比,PD-1抑制剂和高PD-L1表达(≥1%或≥50%)与更高的MPR和pCR率相关。
与nCT和nICI单药治疗相比,nICI联合治疗的MPR和pCR率更高。PD-1抑制剂似乎优于PD-L1抑制剂。PD-L1状态似乎可预测接受nICI治疗患者的MPR和pCR。
https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=278661,CRD42021278661。