Gambaro Alessia, Lombardi Gianmarco, Caletti Chiara, Ribichini Flavio Luciano, Ferraro Pietro Manuel, Gambaro Giovanni
Division of Cardiology, Department of Medicine, University of Verona, 37126 Verona, Italy.
Division of Nephrology, Department of Medicine, University of Verona, 37126 Verona, Italy.
J Clin Med. 2022 Sep 20;11(19):5512. doi: 10.3390/jcm11195512.
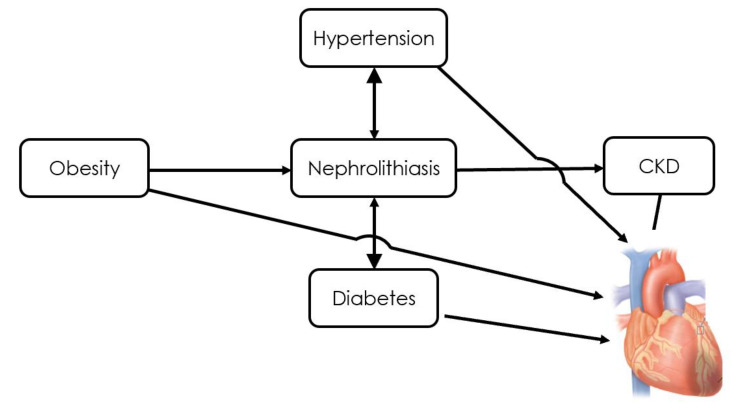
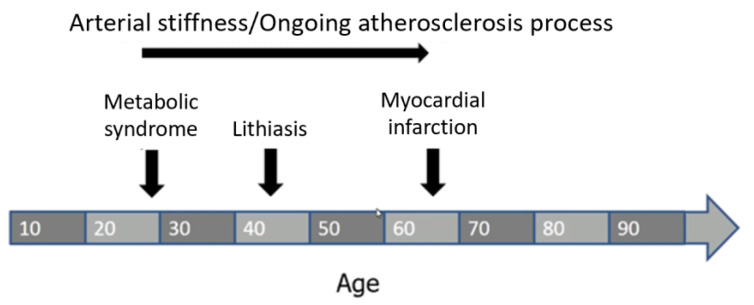
Epidemiological evidence shows that nephrolithiasis is associated with cardiovascular (CV) morbidities. The association between nephrolithiasis and CV disease is not surprising because both diseases share conditions that facilitate their development. Metabolic conditions, encompassed in the definition of metabolic syndrome (MS), and habits that promote nephrolithiasis by altering urine composition also promote clinical manifestations of CV disease. By inducing oxidative stress, these conditions cause endothelial dysfunction and increased arterial stiffness, which are both well-known predictors of CV disease. Furthermore, the subtle systemic metabolic acidosis observed in stone formers with CV disease may have a pathogenic role by increasing bone turnover and leading to reduced mineral content and osteoporosis/osteopenia. Heart valves and/or coronary artery and aortic calcifications are frequently associated with reduced mineral density. This is known as the 'calcification paradox' in osteoporosis and has also been observed in subjects with calcium nephrolithiasis. Evidence supports the hypothesis that osteoporosis/osteopenia is an independent risk factor for the development of CV calcifications. In the long term, episodes of renal stones may occur from the onset of metabolic derangements/MS to arterial stiffness/atherosclerosis and CV morbidities. These episodes should be considered a warning sign of an ongoing and silent atherosclerotic process. The evaluation of cardiometabolic risk factors and MS components should be routine in the assessment of renal stone formers. This would allow for treatment and prevention of the development of CV complications, which are much more severe for the patient and for public health.
流行病学证据表明,肾结石与心血管疾病相关。肾结石与心血管疾病之间的关联并不令人惊讶,因为这两种疾病都有促进其发展的共同条件。代谢综合征(MS)定义中包含的代谢状况,以及通过改变尿液成分促进肾结石形成的习惯,也会促进心血管疾病的临床表现。通过诱导氧化应激,这些状况会导致内皮功能障碍和动脉僵硬度增加,而这两者都是心血管疾病的众所周知的预测指标。此外,在患有心血管疾病的结石形成者中观察到的轻微全身性代谢性酸中毒,可能通过增加骨转换并导致矿物质含量降低和骨质疏松症/骨质减少而发挥致病作用。心脏瓣膜和/或冠状动脉及主动脉钙化常与矿物质密度降低相关。这在骨质疏松症中被称为“钙化悖论”,在钙结石患者中也有观察到。有证据支持骨质疏松症/骨质减少是心血管钙化发展的独立危险因素这一假说。从长远来看,从代谢紊乱/代谢综合征发作到动脉僵硬度增加/动脉粥样硬化和心血管疾病,可能会出现肾结石发作。这些发作应被视为正在进行的无症状动脉粥样硬化过程的警示信号。在评估肾结石患者时,应常规评估心脏代谢危险因素和代谢综合征成分。这将有助于治疗和预防心血管并发症的发生,而心血管并发症对患者和公众健康的影响要严重得多。