Department of Epidemiology, Mailman School of Public Heath Columbia University Irving Medical Center New York NY.
Department of Medicine, Brigham and Women's Hospital and Beth Israel Deaconess Medical Center Harvard Medical School Boston MA.
J Am Heart Assoc. 2022 Nov;11(21):e025252. doi: 10.1161/JAHA.122.025252. Epub 2022 Oct 19.
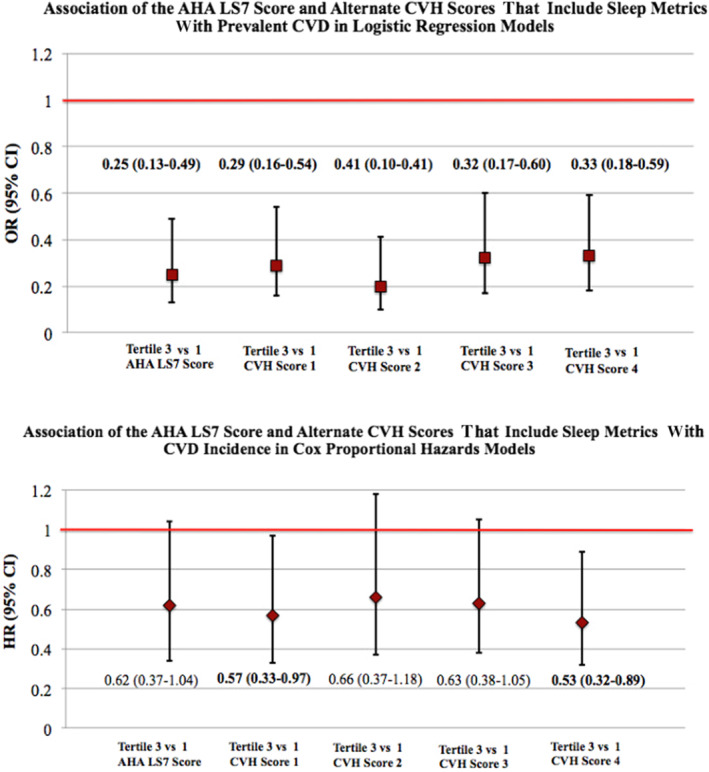
Background Although sufficient and healthy sleep is inversely associated with cardiovascular disease (CVD) and its risk factors, the American Heart Association's Life's Simple 7 (LS7), as a measure of cardiovascular health (CVH), did not include sleep. We evaluated an expanded measure of CVH that includes sleep as an eighth metric in relation to CVD risk. Methods and Results The analytic sample consisted of MESA (Multi-Ethnic Study of Atherosclerosis) Sleep Study participants who had complete data on sleep characteristics from overnight polysomnography, 7-day wrist actigraphy, validated questionnaires, and the outcome. We computed the LS7 score and 4 iterations of a new CVH score: score 1 included sleep duration, score 2 included sleep characteristics linked to CVD in the literature (sleep duration, insomnia, daytime sleepiness, and obstructive sleep apnea), scores 3 and 4 included sleep characteristics associated with CVD in MESA (score 3: sleep duration and efficiency, daytime sleepiness, and obstructive sleep apnea; score 4: score 3+sleep regularity). Multivariable-adjusted logistic and Cox proportional hazards models evaluated associations of the LS7 and CVH scores 1 to 4 with CVD prevalence and incidence. Among 1920 participants (mean age: 69±9 years; 54% female), there were 95 prevalent CVD events and 93 incident cases (mean follow-up, 4.4 years). Those in the highest versus lowest tertile of the LS7 score and CVH scores 1 to 4 had up to 80% lower odds of prevalent CVD. The LS7 score was not significantly associated with CVD incidence (hazard ratio, 0.62 [95% CI, 0.37-1.04]). Those in the highest versus lowest tertile of CVH score 1, which included sleep duration, and CVH score 4, which included multidimensional sleep health, had 43% and 47% lower incident CVD risk (hazard ratio, 0.57 [95% CI, 0.33-0.97]; and hazard ratio, 0.53 [95% CI, 0.32-0.89]), respectively. Conclusions CVH scores that include sleep health predicted CVD risk in older US adults. The incorporation of sleep as a CVH metric, akin to other health behaviors, may enhance CVD primordial and primary prevention efforts. Findings warrant confirmation in larger cohorts over longer follow-up.
尽管充足和健康的睡眠与心血管疾病(CVD)及其危险因素呈负相关,但美国心脏协会的生命简单 7 项(LS7)作为心血管健康(CVH)的衡量标准,并未包含睡眠。我们评估了一种扩展的 CVH 衡量标准,该标准将睡眠作为第八项指标纳入与 CVD 风险相关的研究中。
分析样本由 MESA(动脉粥样硬化多民族研究)睡眠研究参与者组成,这些参与者的睡眠特征数据完整,包括夜间多导睡眠图、7 天腕部活动记录仪、经过验证的问卷和结果。我们计算了 LS7 评分和 4 种新的 CVH 评分:评分 1 包括睡眠时间,评分 2 包括与文献中 CVD 相关的睡眠特征(睡眠时间、失眠、白天嗜睡和阻塞性睡眠呼吸暂停),评分 3 和 4 包括与 MESA 中 CVD 相关的睡眠特征(评分 3:睡眠时间和效率、白天嗜睡和阻塞性睡眠呼吸暂停;评分 4:评分 3+睡眠规律性)。多变量调整的逻辑和 Cox 比例风险模型评估了 LS7 和 CVH 评分 1 至 4 与 CVD 患病率和发病率之间的关联。在 1920 名参与者中(平均年龄:69±9 岁;54%为女性),有 95 例现患 CVD 事件和 93 例新发病例(平均随访 4.4 年)。LS7 评分和 CVH 评分 1 至 4 的最高三分位与最低三分位相比,现患 CVD 的可能性分别降低了 80%。LS7 评分与 CVD 发病率无显著相关性(风险比,0.62 [95%CI,0.37-1.04])。LS7 评分 1 中最高与最低三分位的参与者和 CVH 评分 4 中包含多维睡眠健康的参与者,其新发 CVD 风险分别降低了 43%和 47%(风险比,0.57 [95%CI,0.33-0.97];和风险比,0.53 [95%CI,0.32-0.89])。
包含睡眠健康的 CVH 评分可预测美国老年人的 CVD 风险。将睡眠纳入 CVH 衡量标准,类似于其他健康行为,可以增强 CVD 原始和一级预防措施。这些发现需要在更长的随访时间内,通过更大的队列来确认。