Tayek John A, Stolz Andrew A, Nguyen Danh V, Fleischman M Wayne, Donovan John A, Alcorn Joseph M, Chao Daniel C-K, Asghar Aliya, Morgan Timothy R
Department of Medicine, Harbor-UCLA Medical Center and Lundquist Institute, Torrance, CA, United States.
LAC-USC Medical Center, Los Angeles, CA and the Hepatology Section, Division of Medicine, University of Southern California, Los Angeles, CA, United States.
EClinicalMedicine. 2022 Oct 12;54:101689. doi: 10.1016/j.eclinm.2022.101689. eCollection 2022 Dec.
In trials conducted in India, recombinant granulocyte colony stimulating factor (GCSF) improved survival in alcohol-associated hepatitis (AH). The aim of this trial was to determine the safety and efficacy of pegfilgrastim, a long-acting recombinant GCSF, in patients with AH in the United States.
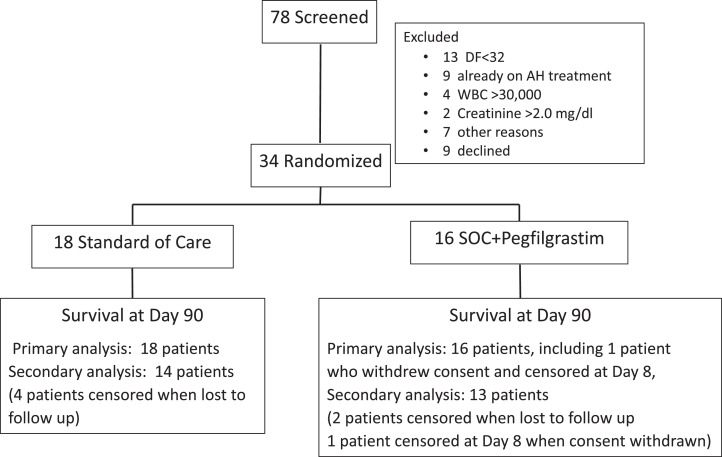
This prospective, randomized, open label trial conducted between March 2017 and March 2020 randomized patients with a clinical diagnosis of AH and a Maddrey discriminant function score ≥32 to standard of care (SOC) or SOC+pegfilgrastim (0.6 mg subcutaneously) on Day 1 and Day 8 (clinicaltrials.gov NCT02776059). SOC was 28 days of either pentoxifylline or prednisolone, as determined by the patient's primary physician. The second injection of pegfilgrastim was not administered if the white blood cell count exceeded 30,000/mm on Day 8. Primary outcome was survival at Day 90. Secondary outcomes included the incidence of acute kidney injury (AKI), hepatorenal syndrome (HRS), hepatic encephalopathy, or infections.
The study was terminated early due to COVID19 pandemic. Eighteen patients were randomized to SOC and 16 to SOC+pegfilgrastim. All patients received prednisolone as SOC. Nine patients failed to receive a second dose of pegfilgrastin due to WBC > 30,000/mm on Day 8. Survival at 90 days was similar in both groups (SOC: 0.83 [95% confidence interval [CI]: 0.57-0.94] vs. pegfilgrastim: 0.73 [95% CI: 0.44-0.89]; p > 0.05; CI for difference: -0.18-0.38). The incidences of AKI, HRS, hepatic encephalopathy, and infections were similar in both treatment arms and there were no serious adverse events attributed to pegfilgrastim.
This phase II trial found no survival benefit at 90 days among subjects with AH who received pegfilgrastim+prednisolone compared with subjects receiving prednisolone alone.
was provided by the United States National Institutes of Health and National Institute on Alcohol Abuse and Alcoholism U01-AA021886 and U01-AA021884.
在印度进行的试验中,重组粒细胞集落刺激因子(GCSF)可提高酒精性肝炎(AH)患者的生存率。本试验的目的是确定聚乙二醇化非格司亭(一种长效重组GCSF)在美国AH患者中的安全性和有效性。
这项前瞻性、随机、开放标签试验于2017年3月至2020年3月进行,将临床诊断为AH且Maddrey判别函数评分≥32的患者随机分为标准治疗(SOC)组或SOC+聚乙二醇化非格司亭组(第1天和第8天皮下注射0.6mg)(clinicaltrials.gov NCT02776059)。SOC为患者的主治医生确定的28天己酮可可碱或泼尼松龙治疗。如果第8天白细胞计数超过30,000/mm³,则不进行第二次聚乙二醇化非格司亭注射。主要结局是第90天的生存率。次要结局包括急性肾损伤(AKI)、肝肾综合征(HRS)、肝性脑病或感染的发生率。
该研究因COVID-19大流行而提前终止。18名患者被随机分配至SOC组,16名患者被随机分配至SOC+聚乙二醇化非格司亭组。所有患者均接受泼尼松龙作为SOC治疗。9名患者因第8天白细胞计数>30,000/mm³而未接受第二剂聚乙二醇化非格司亭。两组90天生存率相似(SOC组:0.83[95%置信区间[CI]:0.57-0.94],聚乙二醇化非格司亭组:0.73[95%CI:0.44-0.89];p>0.05;差异CI:-0.18-0.38)。AKI、HRS、肝性脑病和感染的发生率在两个治疗组中相似,且没有归因于聚乙二醇化非格司亭的严重不良事件。
这项II期试验发现,与单独接受泼尼松龙治疗的受试者相比,接受聚乙二醇化非格司亭+泼尼松龙治疗的AH受试者在90天时没有生存获益。
由美国国立卫生研究院和国家酒精滥用与酒精中毒研究所提供,资助编号为U01-AA021886和U01-AA021884。