ICES, Toronto, ON M4N 3M5, Canada.
Institute of Health Policy, Management, and Evaluation, University of Toronto, Toronto, ON M5T 3M6, Canada.
Curr Oncol. 2022 Oct 14;29(10):7732-7744. doi: 10.3390/curroncol29100611.
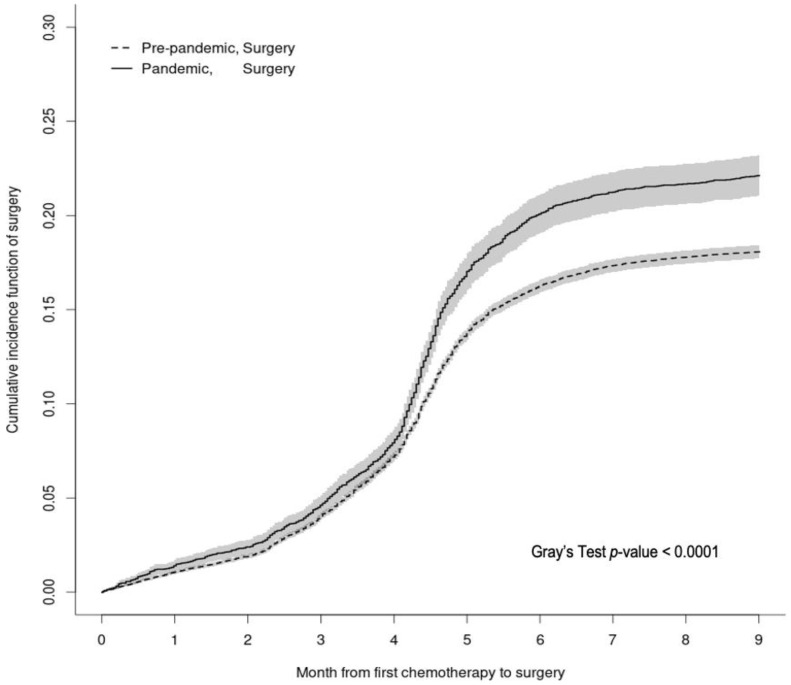
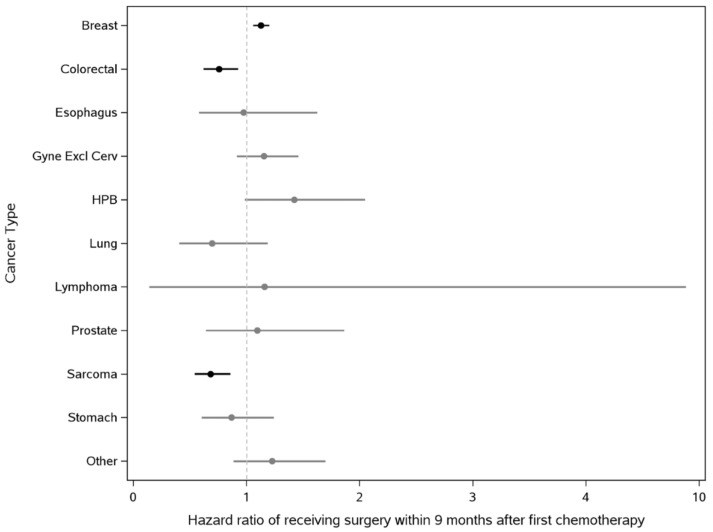
Due to the ramping down of cancer surgery in early pandemic, many newly diagnosed patients received other treatments first. We aimed to quantify the pandemic-related shift in rate of surgery following chemotherapy. This is a retrospective population-based cohort study involving adults diagnosed with cancer between 3 January 2016 and 7 November 2020 in Ontario, Canada who received chemotherapy as first treatment within 6-months of diagnosis. Competing-risks regression models with interaction effects were used to quantify the association between COVID-19 period (receiving a cancer diagnosis before or on/after 15 March 2020) and receipt of surgical reSection 9-months after first chemotherapy. Among 51,653 patients, 8.5% ( = 19,558) of them ultimately underwent surgery 9-months after chemotherapy initiation. Receipt of surgery was higher during the pandemic than before (sHR 1.07, 95% CI 1.02-1.13). Material deprivation was independently associated with lower receipt of surgery (least vs. most deprived quintile: sHR 1.11, 95% CI 1.04-1.17), but did not change with the pandemic. The surgical rate increase was most pronounced for breast cancer (sHR 1.13, 95% CI 1.06-1.20). These pandemic-related shifts in cancer treatment requires further evaluations to understand the long-term consequences. Persistent material deprivation-related inequity in cancer surgical access needs to be addressed.
由于大流行早期癌症手术的减少,许多新诊断的患者首先接受了其他治疗。我们旨在量化与大流行相关的化疗后手术率的变化。这是一项回顾性基于人群的队列研究,涉及 2016 年 1 月 3 日至 2020 年 11 月 7 日期间在加拿大安大略省诊断患有癌症的成年人,他们在诊断后 6 个月内接受化疗作为首次治疗。使用具有交互作用的竞争风险回归模型来量化 COVID-19 期间(在 2020 年 3 月 15 日之前或在 3 月 15 日或之后接受癌症诊断)与首次化疗后 9 个月接受手术切除之间的关联。在 51653 名患者中,最终有 8.5%(=19558)的患者在化疗开始后 9 个月接受了手术。大流行期间接受手术的比例高于大流行前(sHR 1.07,95%CI 1.02-1.13)。物质剥夺与接受手术的可能性降低独立相关(最贫穷与最富裕五分位数相比:sHR 1.11,95%CI 1.04-1.17),但不受大流行影响。乳腺癌的手术率增加最为明显(sHR 1.13,95%CI 1.06-1.20)。这些与大流行相关的癌症治疗方式的转变需要进一步评估,以了解其长期后果。需要解决与物质剥夺相关的癌症手术机会不平等问题。