Marquardt Lynn, Craven Alexander R, Hugdahl Kenneth, Johnsen Erik, Kroken Rune Andreas, Kusztrits Isabella, Specht Karsten, Thomassen Anne Synnøve, Weber Sarah, Hirnstein Marco
Department of Biological and Medical Psychology, University of Bergen, 5009 Bergen, Norway.
NORMENT Center of Excellence, University of Bergen and Haukeland University Hospital, 5009 Bergen, Norway.
Brain Sci. 2022 Oct 12;12(10):1382. doi: 10.3390/brainsci12101382.
Transcranial direct current stimulation (tDCS) is used as treatment for auditory verbal hallucinations (AVH). The theory behind the treatment is that tDCS activity in prefrontal cognitive control areas, which are assumed to be active, and simultaneously activity in temporal speech perception areas, which are assumed to be active during AVH. We tested this hypofrontal/hypertemporal reversal theory by investigating anatomical, neurotransmitter, brain activity, and network connectivity changes over the course of tDCS treatment.
A double-blind, randomized controlled trial was conducted with 21 patients receiving either sham or real tDCS treatment (2 mA) twice daily for 5 days. The anode was placed over the left dorsolateral prefrontal cortex (DLPFC) and the cathode over the left temporo-parietal cortex (TPC). Multimodal neuroimaging as well as clinical and neurocognitive functioning assessment were performed before, immediately after, and three months after treatment.
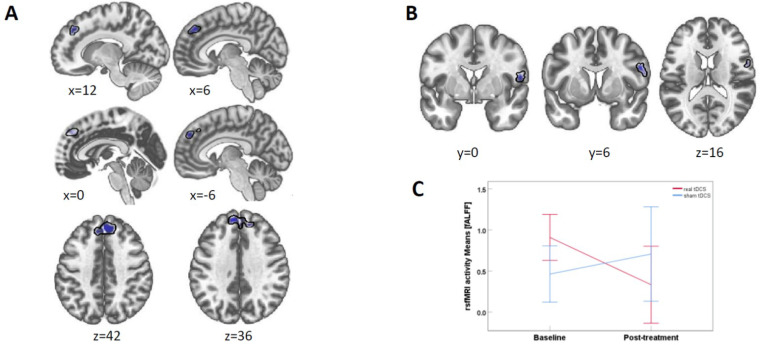
We found a small reduction in AVH severity in the real tDCS group, but no corresponding neuroimaging changes in either DLPFCD or TPC.
The study has a small sample size.
The results suggest that the currently leading theory behind tDCS treatment of AVH may need to be revised, if confirmed by studies with larger N. Tentative findings point to the involvement of Broca's area as a critical structure for tDCS treatment.
经颅直流电刺激(tDCS)被用作治疗幻听(AVH)的方法。该治疗背后的理论是,tDCS可调节前额叶认知控制区域的活动(这些区域被认为在幻听期间是活跃的),同时调节颞叶言语感知区域的活动(这些区域在幻听期间也被认为是活跃的)。我们通过研究tDCS治疗过程中的解剖学、神经递质、脑活动和网络连接变化,对这种前额叶功能减退/颞叶功能亢进反转理论进行了测试。
进行了一项双盲、随机对照试验,21名患者每天接受两次假刺激或真正的tDCS治疗(2毫安),持续5天。阳极置于左侧背外侧前额叶皮质(DLPFC)上方,阴极置于左侧颞顶叶皮质(TPC)上方。在治疗前、治疗后立即以及治疗后三个月进行多模态神经影像学检查以及临床和神经认知功能评估。
我们发现真正的tDCS组幻听严重程度有小幅降低,但DLPFC或TPC均未出现相应的神经影像学变化。
该研究样本量较小。
结果表明,如果更大样本量的研究证实,目前tDCS治疗幻听背后的主导理论可能需要修正。初步研究结果表明,布洛卡区的参与是tDCS治疗的关键结构。