State Key Laboratory of Genetic Engineering and Collaborative Innovation Center for Genetics and Development, School of Life Sciences, Institute of Biomedical Sciences, Human Phenome Institute, Zhongshan Hospital, Fudan University, Shanghai, China.
Department of Neurosurgery, Huashan Hospital, Shanghai Medical College, Fudan University, Shanghai, China.
Cell Res. 2022 Dec;32(12):1047-1067. doi: 10.1038/s41422-022-00736-5. Epub 2022 Oct 28.
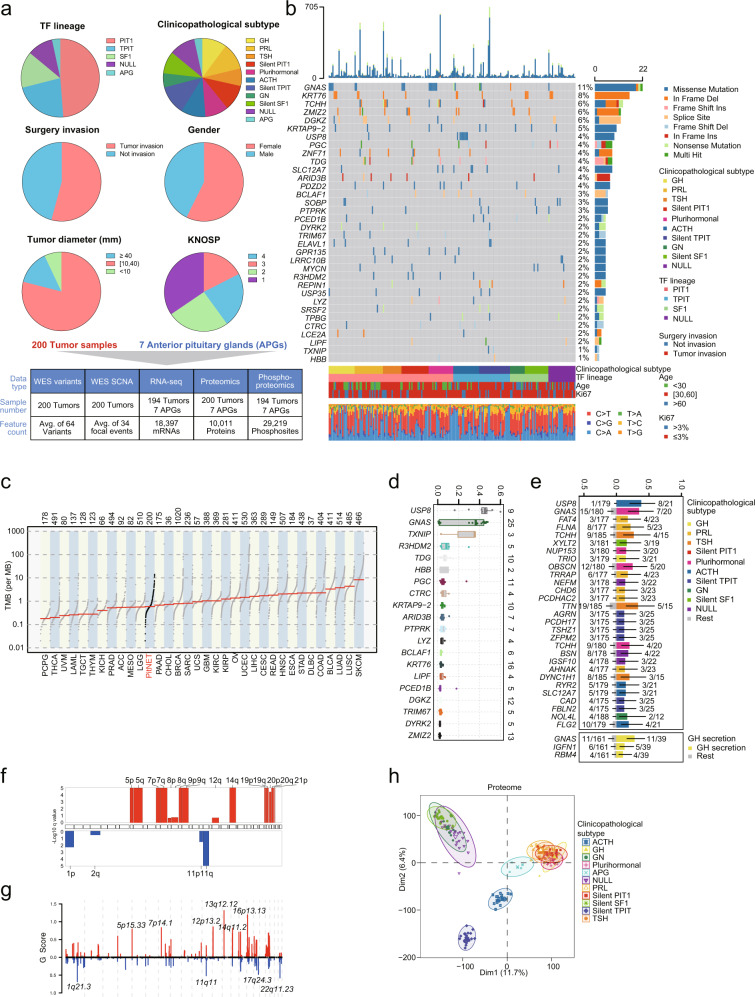
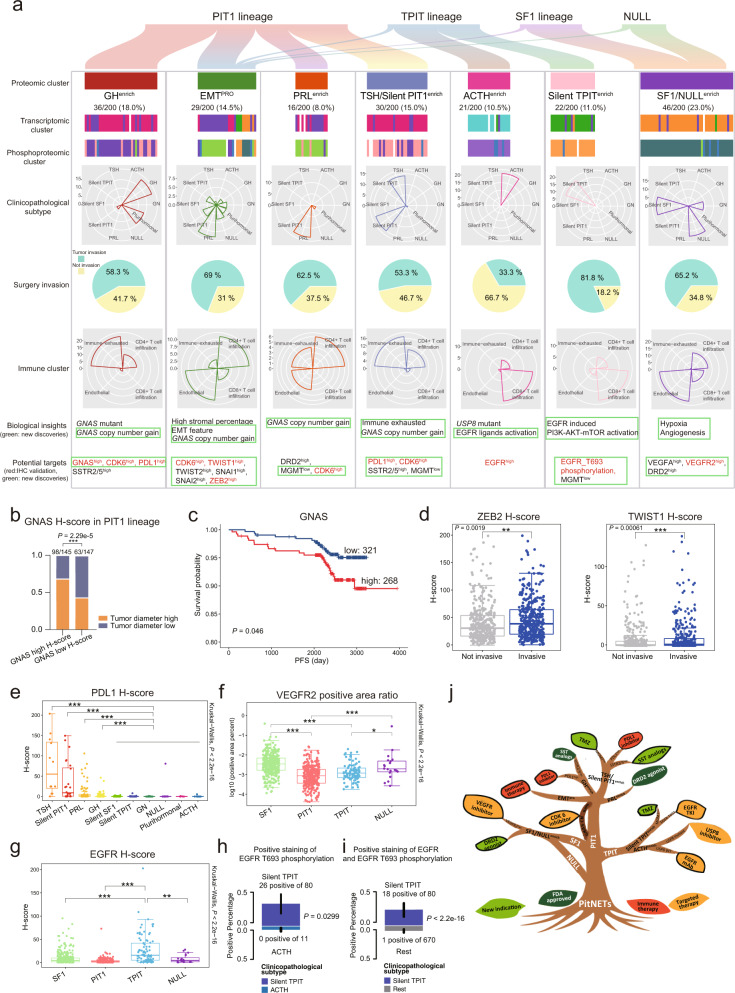
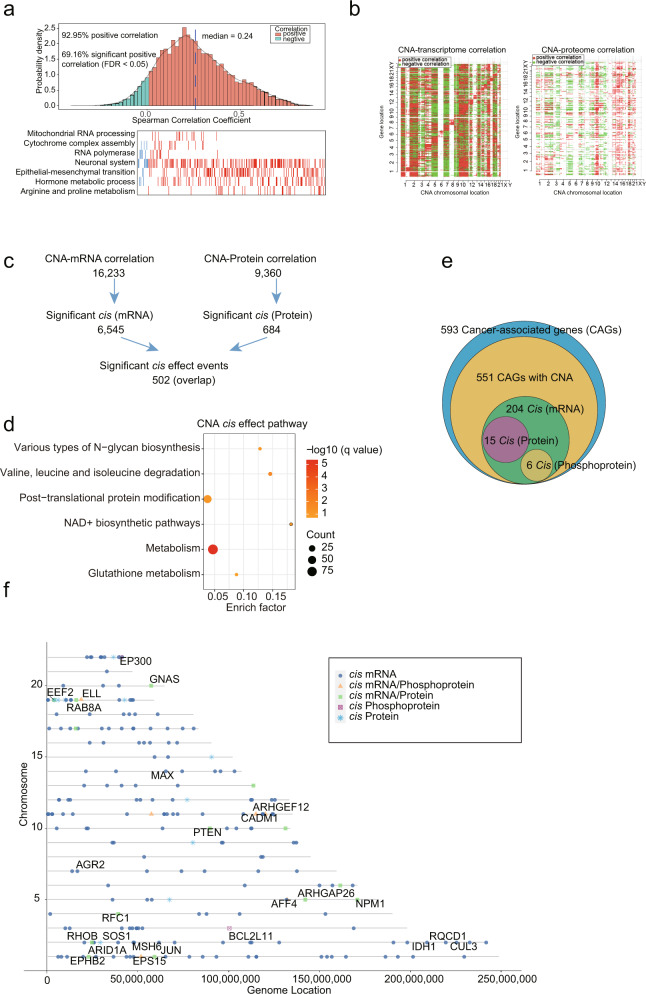
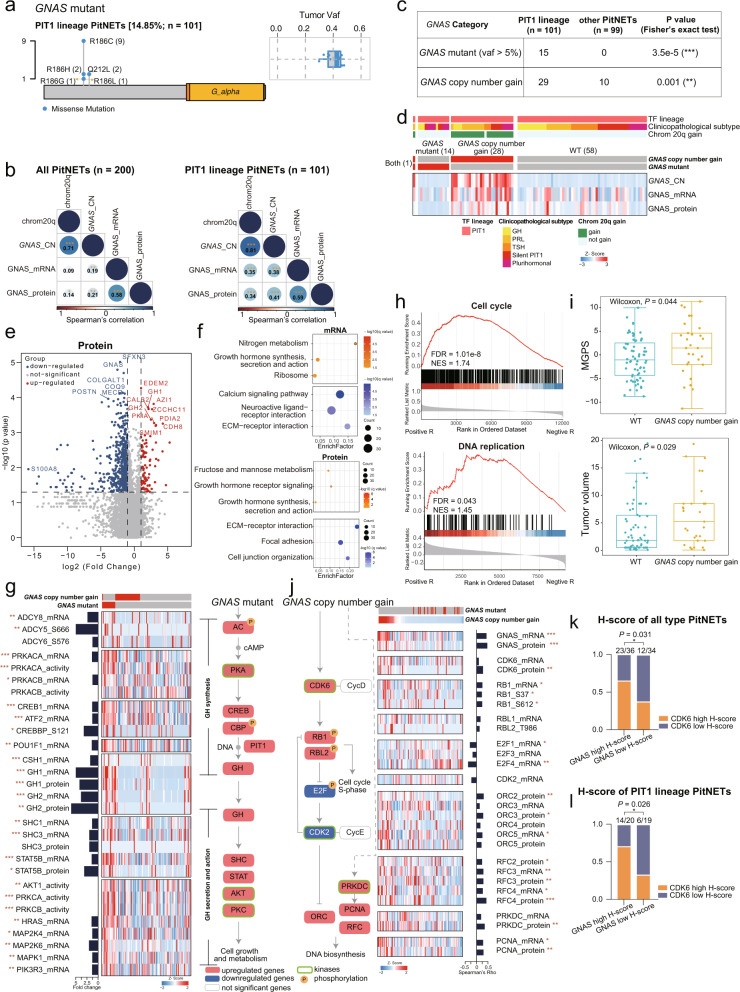
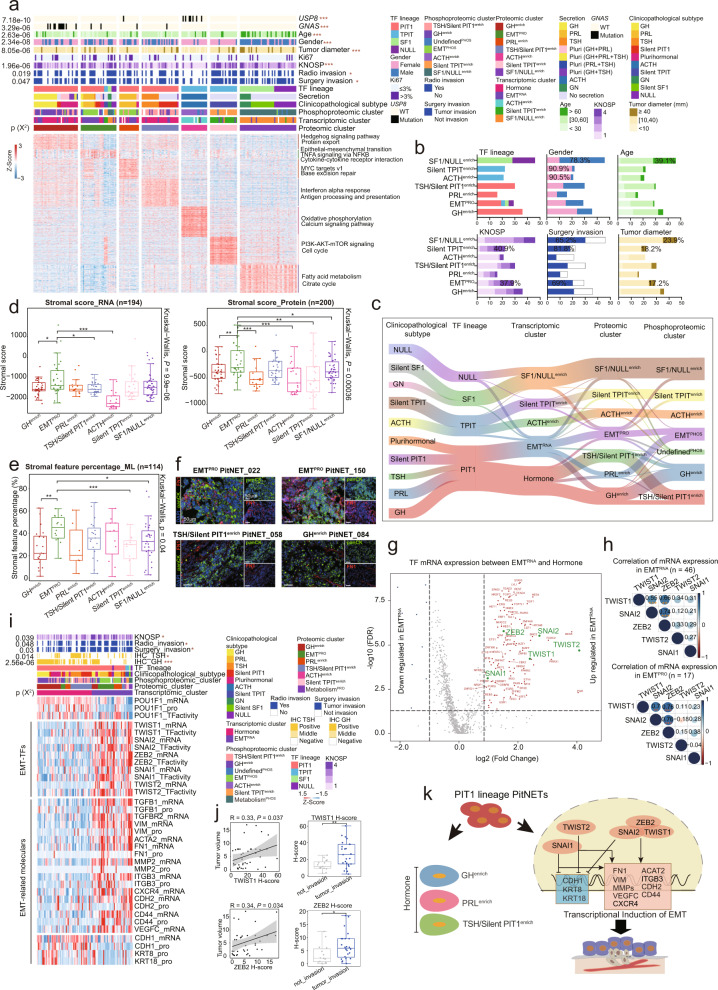
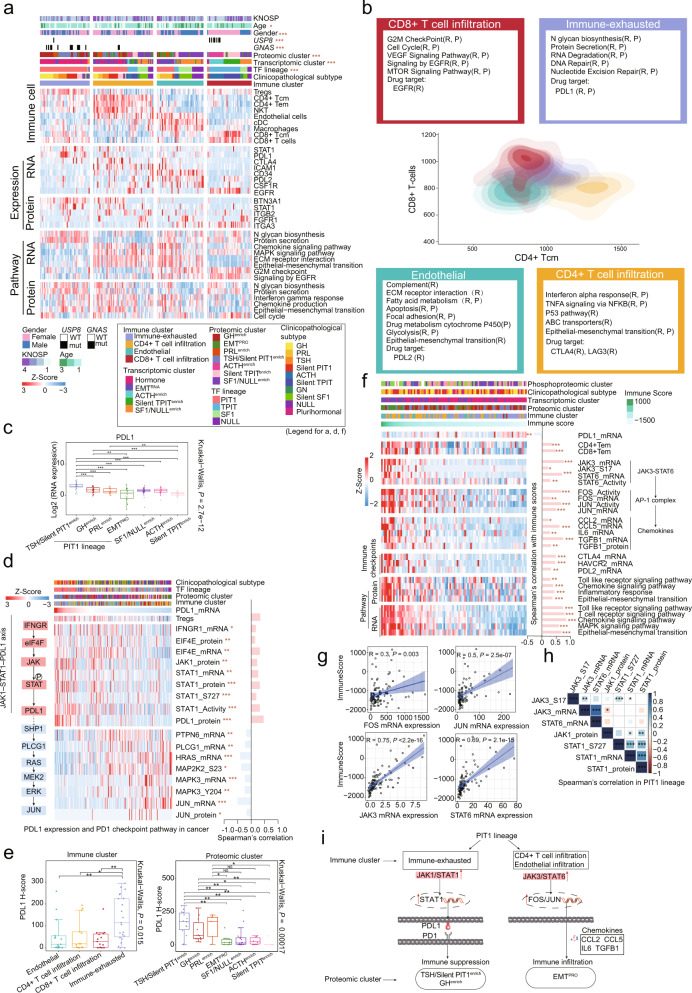
Pituitary neuroendocrine tumor (PitNET) is one of the most common intracranial tumors. Due to its extensive tumor heterogeneity and the lack of high-quality tissues for biomarker discovery, the causative molecular mechanisms are far from being fully defined. Therefore, more studies are needed to improve the current clinicopathological classification system, and advanced treatment strategies such as targeted therapy and immunotherapy are yet to be explored. Here, we performed the largest integrative genomics, transcriptomics, proteomics, and phosphoproteomics analysis reported to date for a cohort of 200 PitNET patients. Genomics data indicate that GNAS copy number gain can serve as a reliable diagnostic marker for hyperproliferation of the PIT1 lineage. Proteomics-based classification of PitNETs identified 7 clusters, among which, tumors overexpressing epithelial-mesenchymal transition (EMT) markers clustered into a more invasive subgroup. Further analysis identified potential therapeutic targets, including CDK6, TWIST1, EGFR, and VEGFR2, for different clusters. Immune subtyping to explore the potential for application of immunotherapy in PitNET identified an association between alterations in the JAK1-STAT1-PDL1 axis and immune exhaustion, and between changes in the JAK3-STAT6-FOS/JUN axis and immune infiltration. These identified molecular markers and alternations in various clusters/subtypes were further confirmed in an independent cohort of 750 PitNET patients. This proteogenomic analysis across traditional histological boundaries improves our current understanding of PitNET pathophysiology and suggests novel therapeutic targets and strategies.
垂体神经内分泌肿瘤(PitNET)是最常见的颅内肿瘤之一。由于其广泛的肿瘤异质性和缺乏用于生物标志物发现的高质量组织,其致病分子机制远未完全确定。因此,需要更多的研究来改进当前的临床病理分类系统,并探索靶向治疗和免疫治疗等先进的治疗策略。在这里,我们对 200 名 PitNET 患者进行了迄今为止最大的综合基因组学、转录组学、蛋白质组学和磷酸化蛋白质组学分析。基因组学数据表明,GNAS 拷贝数增加可作为 PIT1 谱系过度增殖的可靠诊断标志物。基于蛋白质组学的 PitNET 分类确定了 7 个聚类,其中过度表达上皮-间充质转化(EMT)标志物的肿瘤聚类为侵袭性更强的亚组。进一步分析确定了不同聚类的潜在治疗靶点,包括 CDK6、TWIST1、EGFR 和 VEGFR2。免疫亚型分析探索免疫疗法在 PitNET 中的应用潜力,确定了 JAK1-STAT1-PDL1 轴的改变与免疫衰竭之间的关联,以及 JAK3-STAT6-FOS/JUN 轴的改变与免疫浸润之间的关联。在另一个独立的 750 名 PitNET 患者队列中进一步验证了这些鉴定的分子标志物和各种聚类/亚型中的改变。这种跨越传统组织学边界的蛋白质基因组学分析提高了我们对 PitNET 病理生理学的现有认识,并提出了新的治疗靶点和策略。