National Clinical Research Center for Digestive Diseases and Xijing Hospital of Digestive Diseases, Xijing Hospital, Air Force Military Medical University, Xi'anXi'an, 710032, China.
Division of Rheumatology, Allergy and Clinical Immunology, University of California at Davis, Davis, CA, 95616, USA.
Hepatol Int. 2023 Feb;17(1):237-248. doi: 10.1007/s12072-022-10431-7. Epub 2022 Oct 30.
Current treatment guidelines recommend ursodeoxycholic acid (UDCA) as the first-line treatment for new-diagnosed primary biliary cholangitis (PBC) patients. However, up to 40% patients are insensitive to UDCA monotherapy, and evaluation of UDCA response at 12 months may result in long period of ineffective treatment. We aimed to develop a new criterion to reliably identify non-response patients much earlier.
Five hundred sixty-nine patients with an average of 59 months (Median: 53; IQR:32-79) follow-up periods were randomly divided into either the training (70%) or the validation cohort (30%). The efficiency of different combinations of total bilirubin (TBIL), alkaline phosphatase (ALP), and aspartate aminotransferase (AST) threshold values to predict outcomes was assessed at 1, 3 or 6 month after the initiation of UDCA therapy. The endpoints were defined as adverse outcomes, including liver-related death, liver transplantation and complications of cirrhosis. Adverse outcome-free survival was compared using various published criteria and a proposed new criterion.
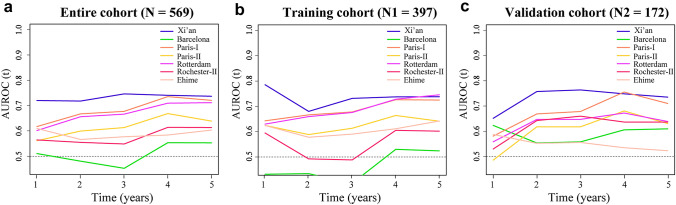
A new criterion of evaluating UDCA responses at 1 month was established as: ALP ≤ 2.5 × upper limit of normal (ULN) and AST ≤ 2 × ULN, and TBIL ≤ 1 × ULN (Xi'an criterion). The 5 year adverse outcome-free survival rate of UDCA responders, defined by Xi'an criterion, was 97%, which was significantly higher than that of those non-responders (64%). An accurate distinguishing high-risk patients' capacity of Xi'an criterion was confirmed in both early and late-stage PBC.
Xi'an criterion has a similar or even higher ability to distinguish high-risk PBC patients than other published criteria. Xi'an criterion can facilitate early identification of patients requiring new therapeutic approaches.
目前的治疗指南建议熊去氧胆酸(UDCA)作为新诊断的原发性胆汁性胆管炎(PBC)患者的一线治疗药物。然而,多达 40%的患者对 UDCA 单药治疗不敏感,并且在 12 个月时评估 UDCA 反应可能导致无效治疗期延长。我们旨在开发一种新的标准,以便更早、更可靠地识别无应答患者。
569 例患者平均随访时间为 59 个月(中位数:53;IQR:32-79),随机分为训练队列(70%)和验证队列(30%)。评估在 UDCA 治疗开始后 1、3 或 6 个月时,总胆红素(TBIL)、碱性磷酸酶(ALP)和天冬氨酸氨基转移酶(AST)截断值的不同组合预测结局的效率。终点定义为肝相关死亡、肝移植和肝硬化并发症等不良结局。使用各种已发表的标准和提出的新标准比较无不良结局的生存率。
建立了一种新的 UDCA 反应评估标准,即 1 个月时:ALP≤2.5×正常上限(ULN)和 AST≤2×ULN,TBIL≤1×ULN(西安标准)。根据西安标准,UDCA 应答者的 5 年无不良结局生存率为 97%,明显高于无应答者(64%)。西安标准在早期和晚期 PBC 中均证实了准确区分高危患者的能力。
西安标准在区分高危 PBC 患者方面具有与其他已发表标准相似或更高的能力。西安标准可以促进早期识别需要新治疗方法的患者。