Massachusetts Veterans Epidemiology Research and Information Center (MAVERIC), VA Boston Healthcare System, Boston, MA (L.G., K.C., R.J.S., D.C.P., P.S., J.J., J.P.C., J.M.G.).
BHF Cardiovascular Epidemiology Unit, Department of Public Health and Primary Care (L.G., L.S., S. Bell, S.K.K., S. Burgess, K.M., A.M.M., T.R.B., E.A., L.C., J.R.S., P.W., L. Pennells, S.H., M.I., J.D., A.S.B., A.M.W., E.D.A.).
Circulation. 2022 Nov 15;146(20):1507-1517. doi: 10.1161/CIRCULATIONAHA.122.060700. Epub 2022 Oct 31.
End-stage renal disease is associated with a high risk of cardiovascular events. It is unknown, however, whether mild-to-moderate kidney dysfunction is causally related to coronary heart disease (CHD) and stroke.
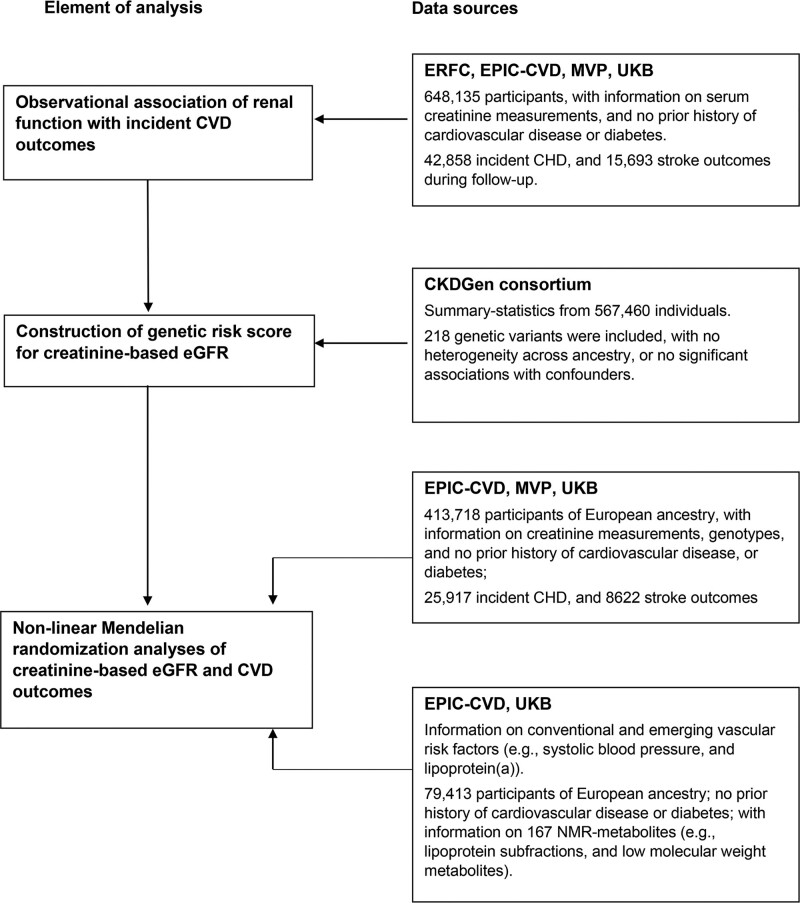
Observational analyses were conducted using individual-level data from 4 population data sources (Emerging Risk Factors Collaboration, EPIC-CVD [European Prospective Investigation into Cancer and Nutrition-Cardiovascular Disease Study], Million Veteran Program, and UK Biobank), comprising 648 135 participants with no history of cardiovascular disease or diabetes at baseline, yielding 42 858 and 15 693 incident CHD and stroke events, respectively, during 6.8 million person-years of follow-up. Using a genetic risk score of 218 variants for estimated glomerular filtration rate (eGFR), we conducted Mendelian randomization analyses involving 413 718 participants (25 917 CHD and 8622 strokes) in EPIC-CVD, Million Veteran Program, and UK Biobank.
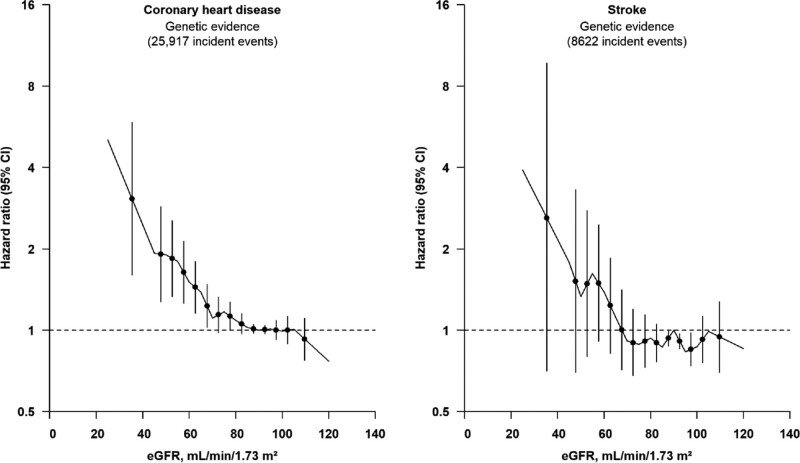
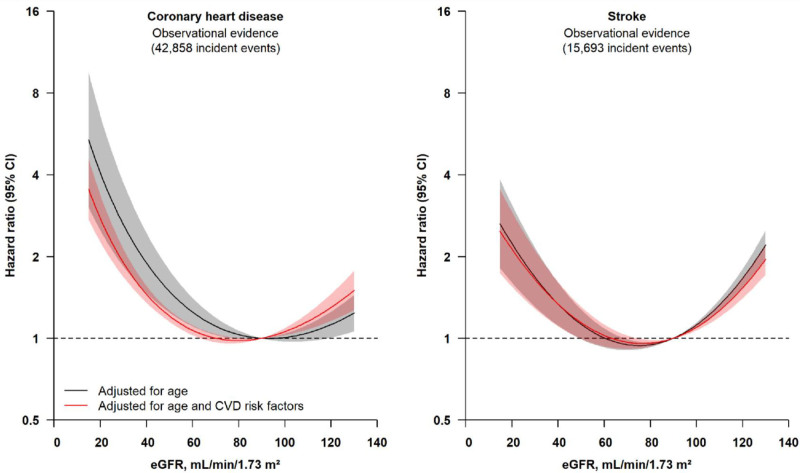
There were U-shaped observational associations of creatinine-based eGFR with CHD and stroke, with higher risk in participants with eGFR values <60 or >105 mL·min·1.73 m, compared with those with eGFR between 60 and 105 mL·min·1.73 m. Mendelian randomization analyses for CHD showed an association among participants with eGFR <60 mL·min·1.73 m, with a 14% (95% CI, 3%-27%) higher CHD risk per 5 mL·min·1.73 m lower genetically predicted eGFR, but not for those with eGFR >105 mL·min·1.73 m. Results were not materially different after adjustment for factors associated with the eGFR genetic risk score, such as lipoprotein(a), triglycerides, hemoglobin A1c, and blood pressure. Mendelian randomization results for stroke were nonsignificant but broadly similar to those for CHD.
In people without manifest cardiovascular disease or diabetes, mild-to-moderate kidney dysfunction is causally related to risk of CHD, highlighting the potential value of preventive approaches that preserve and modulate kidney function.
终末期肾病与心血管事件的高风险相关。然而,轻度至中度肾功能障碍是否与冠心病(CHD)和中风有因果关系尚不清楚。
使用来自 4 个人群数据源(新兴风险因素合作研究、欧洲前瞻性癌症与营养-心血管疾病研究[EPIC-CVD]、百万退伍军人计划和英国生物库)的个体水平数据进行观察性分析,包括 648135 名基线时无心血管疾病或糖尿病史的参与者,在 680 万人年的随访中分别发生了 42858 例和 15693 例 CHD 和中风事件。使用 218 个用于估计肾小球滤过率(eGFR)的遗传风险评分,我们对 EPIC-CVD、百万退伍军人计划和英国生物库中的 413718 名参与者(25917 例 CHD 和 8622 例中风)进行了孟德尔随机化分析。
基于肌酐的 eGFR 与 CHD 和中风呈 U 型观察性关联,与 eGFR 值<60 或>105 mL·min·1.73 m 的参与者相比,eGFR 值<60 或>105 mL·min·1.73 m 的参与者风险更高。对于 CHD,eGFR<60 mL·min·1.73 m 的参与者的孟德尔随机化分析显示,与每降低 5 mL·min·1.73 m 遗传预测 eGFR 相关的 CHD 风险增加 14%(95%CI,3%-27%),但对于 eGFR>105 mL·min·1.73 m 的参与者则不然。调整与 eGFR 遗传风险评分相关的脂蛋白(a)、甘油三酯、血红蛋白 A1c 和血压等因素后,结果没有实质性差异。对于中风的孟德尔随机化结果无统计学意义,但与 CHD 的结果大致相似。
在没有明显心血管疾病或糖尿病的人群中,轻度至中度肾功能障碍与 CHD 风险有因果关系,这突显了保护和调节肾功能的预防方法的潜在价值。