Cardiology Unit, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy.
Department of Specialist, Diagnostic, and Experimental Medicine, Alma Mater Studiorum University of Bologna, Bologna, Italy.
J Cardiothorac Surg. 2022 Nov 1;17(1):280. doi: 10.1186/s13019-022-02027-x.
The diagnosis of periprocedural myocardial infarction (PMI) after coronary artery bypass graft (CABG) is based on biochemical markers along with clinical and instrumental findings. However, there is not a clear cutoff value of high-sensitivity cardiac troponin (hs-cTn) to identify PMI. We hypothesized that isolated hs-cTn concentrations in the first 24 h following CABG could predict cardiac adverse events (in-hospital death and PMI) and/or left ventricular ejection fraction (LVEF) decrease.
We retrospectively enrolled all consecutive adult patients undergoing CABG, alone or in association with other cardiac surgery procedures, over 1 year. Hs-cTn I concentrations (Access, Beckman Coulter) were serially measured in the post-operative period and analyzed according to post-operative outcomes.
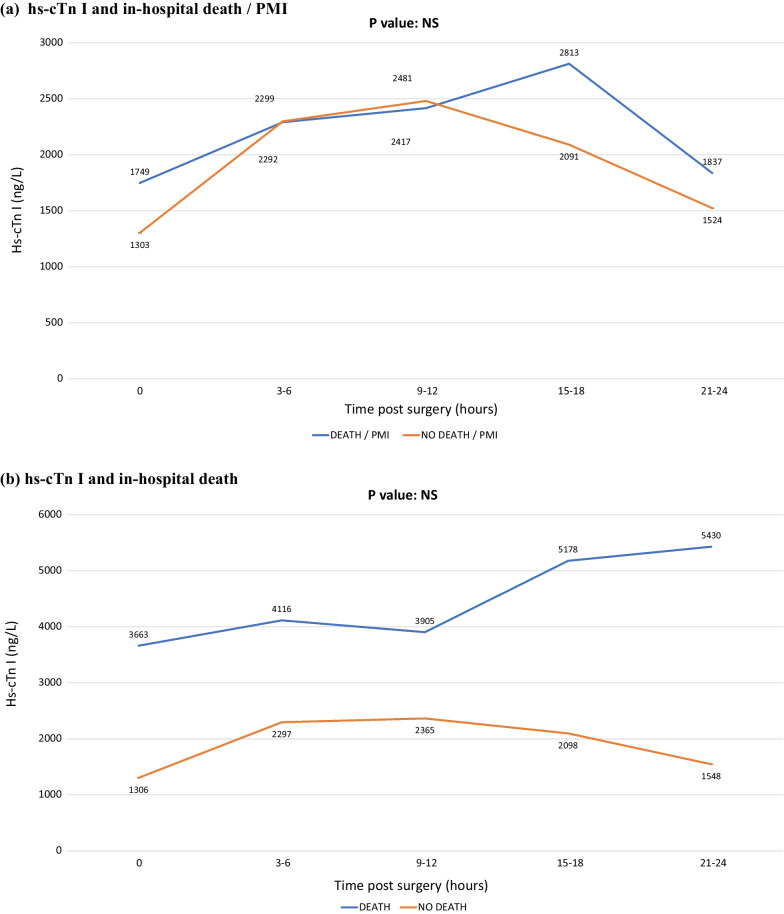
300 patients were enrolled; 71.3% underwent CABG alone, 33.7% for acute coronary syndrome. Most patients showed hs-cTn I values superior to the limit required by the latest guidelines for the diagnosis of PMI. Five patients (1.7%) died, 8% developed a PMI, 10.6% showed a LVEF decrease ≥ 10%. Hs-cTn I concentrations did not significantly differ with respect to death and/or PMI whereas they were associated with LVEF decrease ≥ 10% (p value < 0.005 at any time interval), in particular hs-cTn I values at 9-12 h post-operatively. A hs-cTn I cutoff of 5556 ng/L, a value 281 (for males) and 479 (for females) times higher than the URL, at 9-12 h post-operatively was identified, representing the best balance between sensitivity (55%) and specificity (79%) in predicting LVEF decrease ≥ 10%.
Hs-cTn I at 9-12 h post-CABG may be useful to early identify patients at risk for LVEF decrease and to guide early investigation and management of possible post-operative complications.
冠状动脉旁路移植术(CABG)后围手术期心肌梗死(PMI)的诊断基于生化标志物以及临床和仪器检查结果。然而,目前还没有明确的高敏肌钙蛋白(hs-cTn)截断值来确定 PMI。我们假设 CABG 后 24 小时内孤立的 hs-cTn 浓度可以预测心脏不良事件(院内死亡和 PMI)和/或左心室射血分数(LVEF)下降。
我们回顾性纳入了过去一年中接受 CABG 单独或联合其他心脏手术的所有连续成年患者。术后 hs-cTn I 浓度(Access,贝克曼库尔特)连续测量,并根据术后结果进行分析。
共纳入 300 例患者;71.3%单独接受 CABG,33.7%因急性冠状动脉综合征接受手术。大多数患者的 hs-cTn I 值高于最新指南诊断 PMI 的要求。5 例(1.7%)患者死亡,8%发生 PMI,10.6%出现 LVEF 下降≥10%。hs-cTn I 浓度与死亡和/或 PMI 无显著差异,但与 LVEF 下降≥10%相关(任何时间间隔的 p 值均<0.005),特别是术后 9-12 小时的 hs-cTn I 值。在术后 9-12 小时,我们确定了 hs-cTn I 截断值为 5556ng/L,该值比 URL 高 281 倍(男性)和 479 倍(女性),在预测 LVEF 下降≥10%方面,其敏感性(55%)和特异性(79%)具有最佳平衡。
CABG 后 9-12 小时的 hs-cTn I 可能有助于早期识别 LVEF 下降风险患者,并指导术后可能并发症的早期检查和处理。