Isfordink Cas, Boyd Anders, Mocroft Amanda, Kusejko Katharina, Smit Colette, de Wit Stephane, Mahungu Tabitha, Falconer Karolin, Wandeler Gilles, Cavassini Matthias, Stöckle Marcel, Schinkel Janke, Rauch Andri, Peters Lars, van der Valk Marc
Division of Infectious Diseases, Department of Internal Medicine, Amsterdam Institute for Infection and Immunity, Amsterdam University Medical Center, University of Amsterdam, Amsterdam, The Netherlands.
Department of Gastroenterology and Hepatology, University Medical Centre Utrecht, Utrecht, The Netherlands.
Open Forum Infect Dis. 2022 Sep 30;9(10):ofac508. doi: 10.1093/ofid/ofac508. eCollection 2022 Oct.
Several studies have reported suboptimal efficacy of direct-acting antivirals (DAAs) to treat hepatitis C virus (HCV) subtypes endemic to sub-Saharan Africa (SSA) and Southeastern Asia (SEA). The extent of this issue in individuals with human immunodeficiency virus (HIV)/HCV from SSA or SEA residing in Europe is unknown.
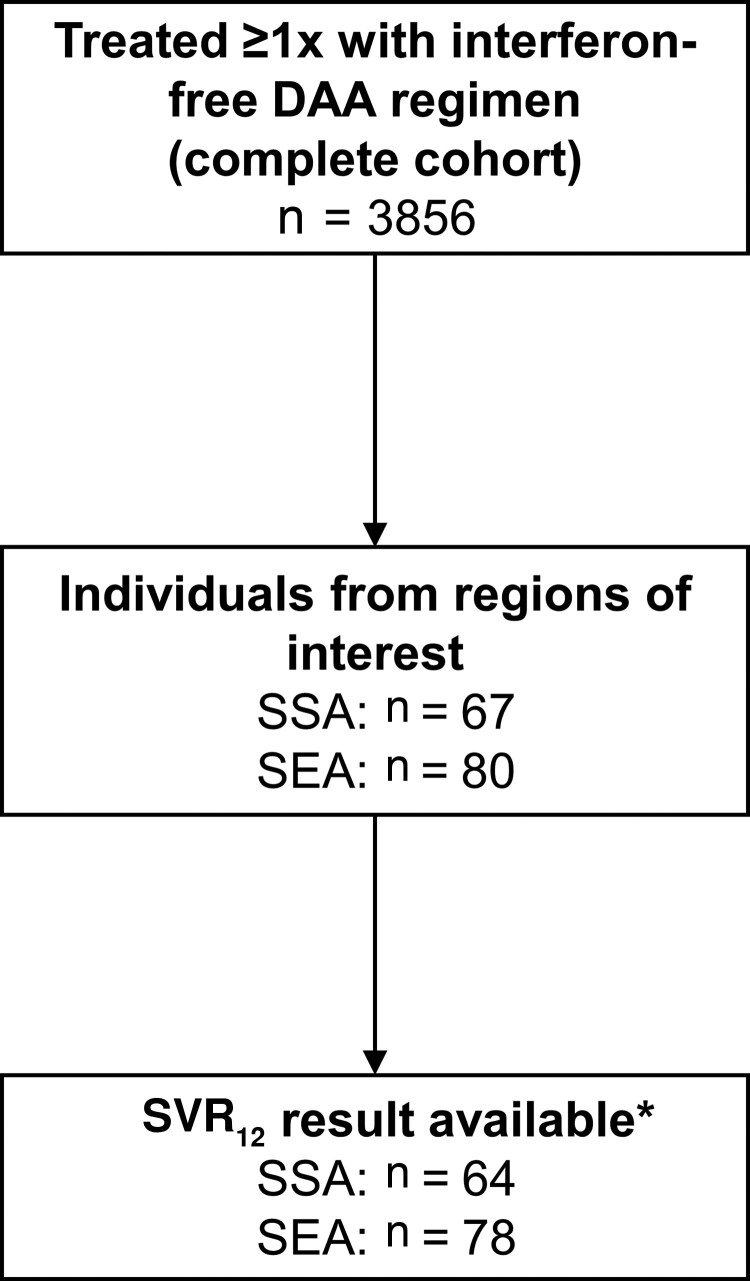
We retrospectively analyzed data from several prospective European cohorts of people living with HIV. We included individuals with HIV/HCV who originated from SSA or SEA, were treated with interferon-free DAAs, and had an available HCV RNA result ≥12 weeks after the end of treatment. The primary outcome was sustained virological response at least 12 weeks after the end of treatment (SVR).
Of the 3293 individuals with HIV/HCV treated with DAA and with available SVR data, 142 were from SSA (n = 64) and SEA (n = 78). SVR was achieved by 60 (94% [95% confidence interval {CI}, 86%-98%]) individuals from SSA and 76 (97% [95% CI, 92%-99%]) from SEA. The genotypes of the 6 individuals failing DAA treatment were 2, 3a, 3h, 4a, 4c, and 6j. For 2 of the 4 unsuccessfully treated individuals with available sequence data at treatment failure, NS5A resistance-associated substitutions were present (30R/93S in an individual with genotype 4c and 31M in an individual with genotype 6j).
SVR rates were high in individuals with HIV/HCV residing in Europe and originating from regions where intrinsically NS5A-resistant HCV strains are endemic. HCV elimination for this population in Europe is unlikely to be hampered by suboptimal DAA efficacy.
多项研究报告称,直接抗病毒药物(DAA)治疗撒哈拉以南非洲(SSA)和东南亚(SEA)流行的丙型肝炎病毒(HCV)亚型的疗效欠佳。在欧洲居住的来自SSA或SEA的人类免疫缺陷病毒(HIV)/HCV感染者中,这一问题的严重程度尚不清楚。
我们回顾性分析了欧洲几个HIV感染者前瞻性队列的数据。我们纳入了来自SSA或SEA、接受无干扰素DAA治疗且在治疗结束后至少12周有可用HCV RNA结果的HIV/HCV感染者。主要结局是治疗结束后至少12周的持续病毒学应答(SVR)。
在3293例接受DAA治疗且有可用SVR数据的HIV/HCV感染者中,142例来自SSA(n = 64)和SEA(n = 78)。来自SSA的60例(94%[95%置信区间{CI},86%-98%])和来自SEA的76例(97%[95%CI,92%-99%])实现了SVR。6例DAA治疗失败的感染者的基因型分别为2、3a、3h、4a、4c和6j。在4例治疗失败且有可用序列数据的未成功治疗感染者中,有2例存在NS5A耐药相关替代(基因型4c感染者为30R/93S,基因型6j感染者为31M)。
居住在欧洲且来自NS5A内在耐药HCV毒株流行地区的HIV/HCV感染者的SVR率较高。欧洲该人群的HCV消除不太可能因DAA疗效欠佳而受阻。