Division of Cardiology, Department of Medicine, University of Pittsburgh Heart and Vascular Institute, Pittsburgh, Pennsylvania.
Division of Hospital Medicine, Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, Maryland.
JAMA Netw Open. 2022 Nov 1;5(11):e2240145. doi: 10.1001/jamanetworkopen.2022.40145.
Direct oral anticoagulant (DOAC)-associated intracranial hemorrhage (ICH) has high morbidity and mortality. The safety and outcome data of DOAC reversal agents in ICH are limited.
To evaluate the safety and outcomes of DOAC reversal agents among patients with ICH.
PubMed, MEDLINE, The Cochrane Library, Embase, EBSCO, Web of Science, and CINAHL databases were searched from inception through April 29, 2022.
The eligibility criteria were (1) adult patients (age ≥18 years) with ICH receiving treatment with a DOAC, (2) reversal of DOAC, and (3) reported safety and anticoagulation reversal outcomes. All nonhuman studies and case reports, studies evaluating patients with ischemic stroke requiring anticoagulation reversal or different dosing regimens of DOAC reversal agents, and mixed study groups with DOAC and warfarin were excluded.
Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines were used for abstracting data and assessing data quality and validity. Two reviewers independently selected the studies and abstracted data. Data were pooled using the random-effects model.
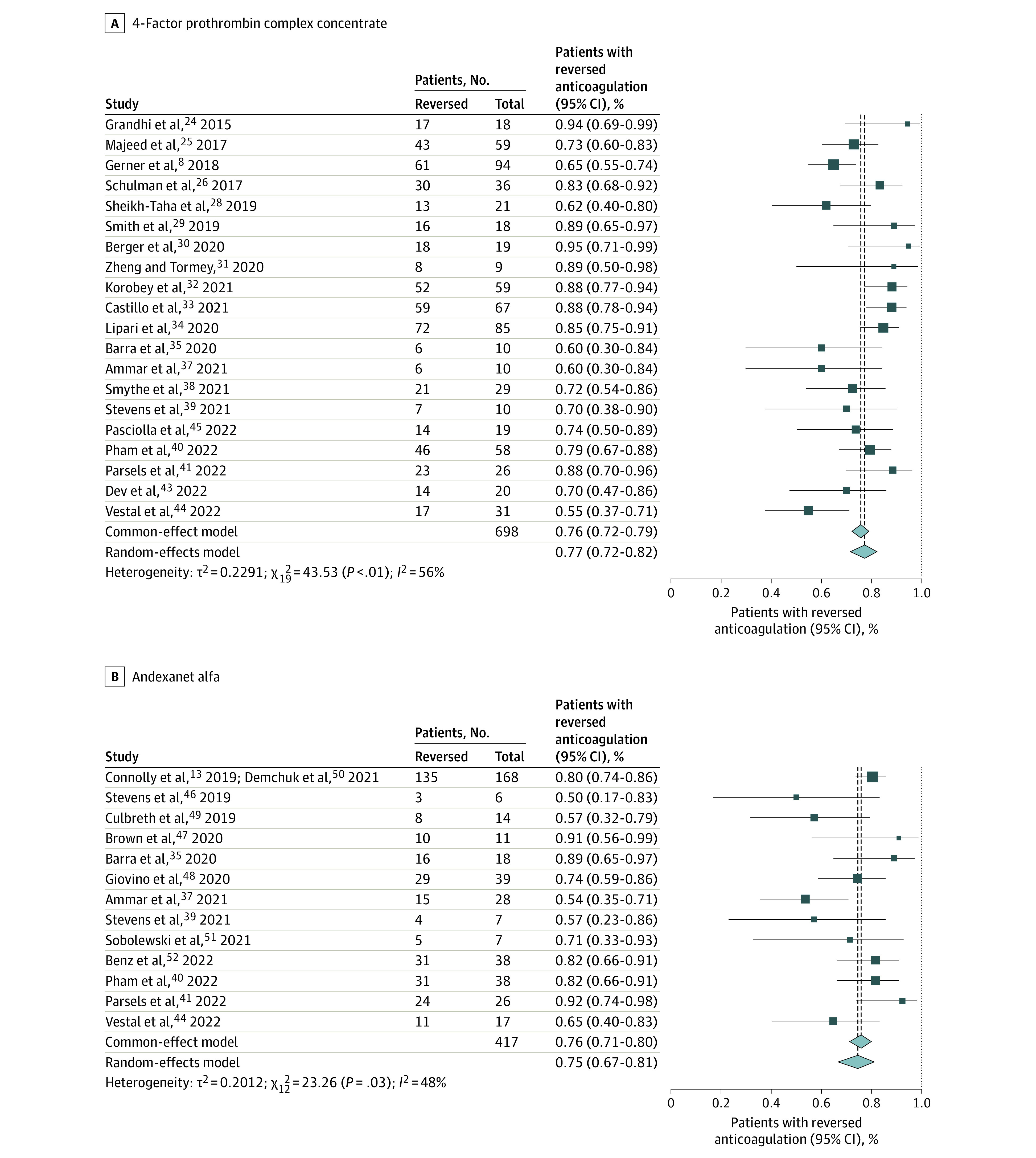
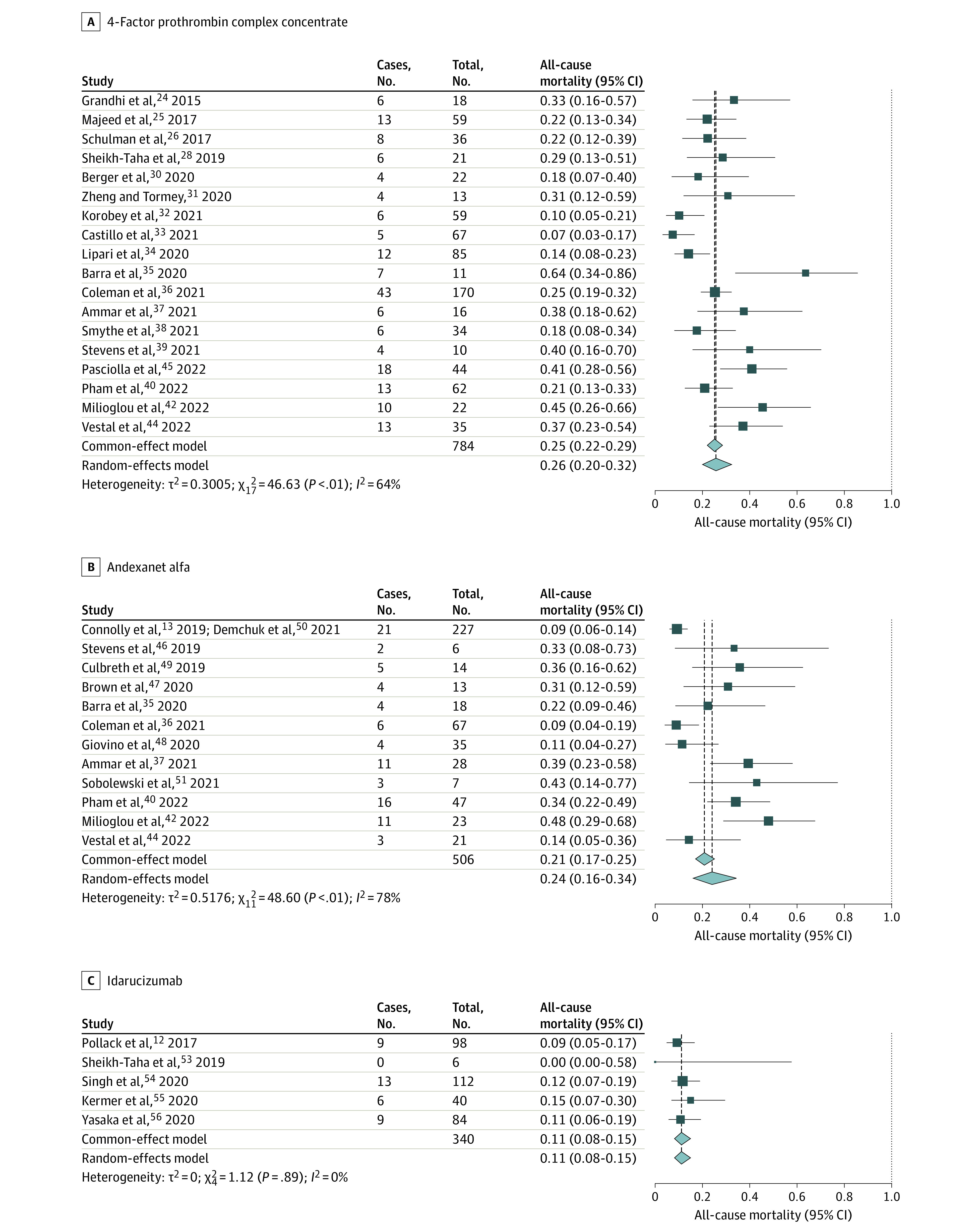
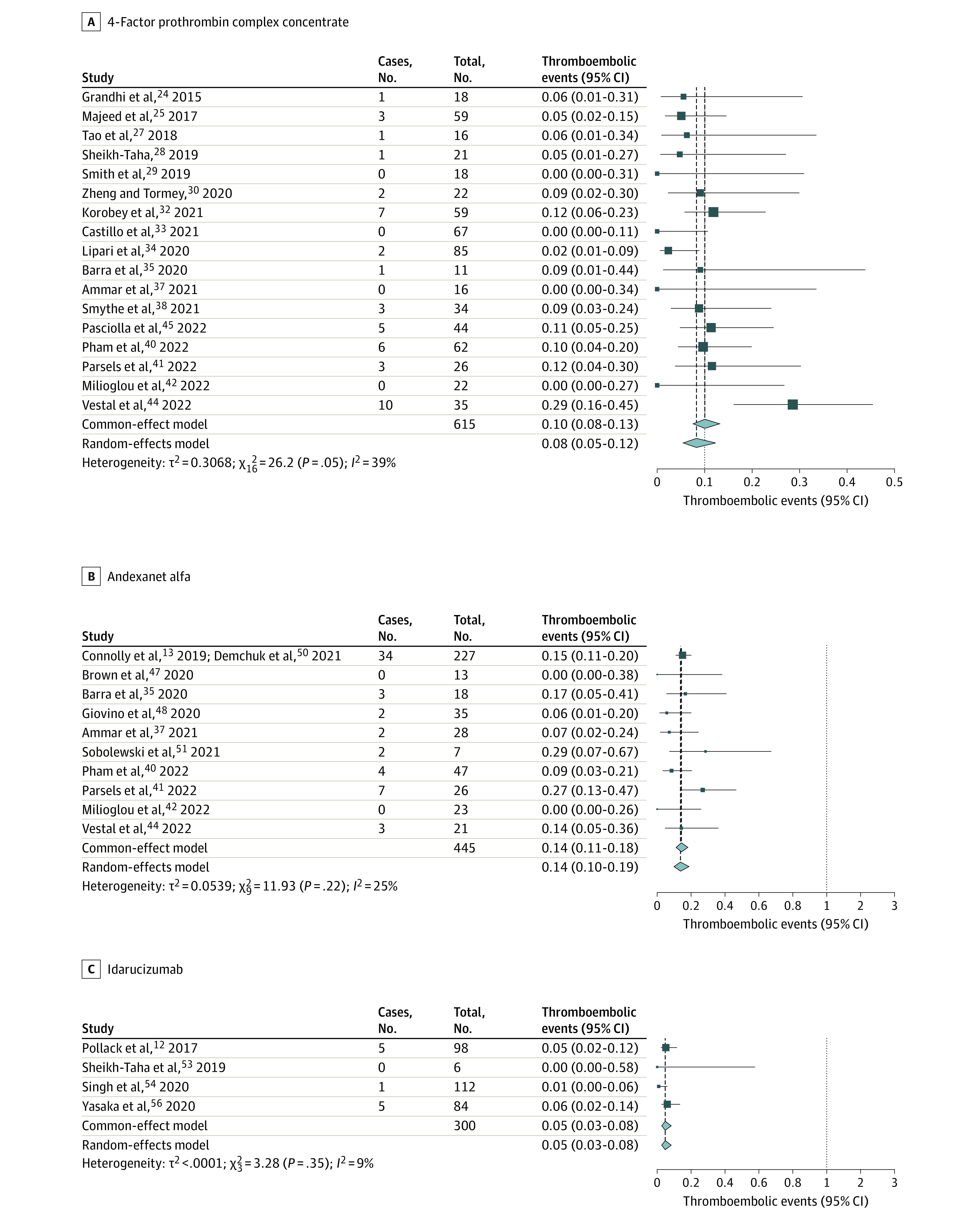
The primary outcome was proportion with anticoagulation reversed. The primary safety end points were all-cause mortality and thromboembolic events after the reversal agent.
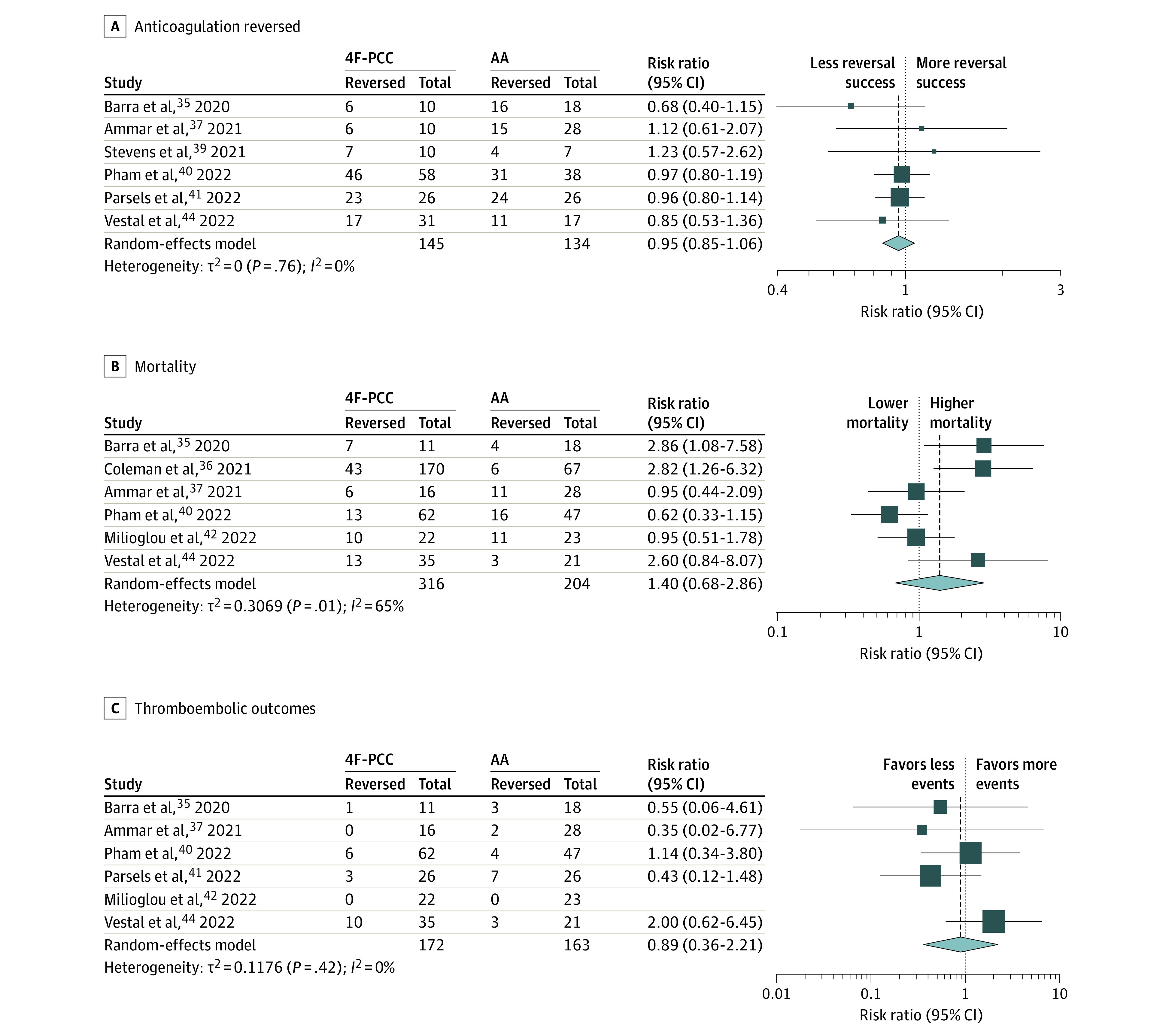
A total of 36 studies met criteria for inclusion, with a total of 1832 patients (967 receiving 4-factor prothrombin complex concentrate [4F-PCC]; 525, andexanet alfa [AA]; 340, idarucizumab). The mean age was 76 (range, 68-83) years, and 57% were men. For 4F-PCC, anticoagulation reversal was 77% (95% CI, 72%-82%; I2 = 55%); all-cause mortality, 26% (95% CI, 20%-32%; I2 = 68%), and thromboembolic events, 8% (95% CI, 5%-12%; I2 = 41%). For AA, anticoagulation reversal was 75% (95% CI, 67%-81%; I2 = 48%); all-cause mortality, 24% (95% CI, 16%-34%; I2 = 73%), and thromboembolic events, 14% (95% CI, 10%-19%; I2 = 16%). Idarucizumab for reversal of dabigatran had an anticoagulation reversal rate of 82% (95% CI, 55%-95%; I2 = 41%), all-cause mortality, 11% (95% CI, 8%-15%, I2 = 0%), and thromboembolic events, 5% (95% CI, 3%-8%; I2 = 0%). A direct retrospective comparison of 4F-PCC and AA showed no differences in anticoagulation reversal, proportional mortality, or thromboembolic events.
In the absence of randomized clinical comparison trials, the overall anticoagulation reversal, mortality, and thromboembolic event rates in this systematic review and meta-analysis appeared similar among available DOAC reversal agents for managing ICH. Cost, institutional formulary status, and availability may restrict reversal agent choice, particularly in small community hospitals.
直接口服抗凝剂(DOAC)相关的颅内出血(ICH)具有高发病率和死亡率。DOAC 逆转剂在 ICH 中的安全性和结果数据有限。
评估 ICH 患者使用 DOAC 逆转剂的安全性和结局。
从建库至 2022 年 4 月 29 日,检索了 PubMed、MEDLINE、The Cochrane Library、Embase、EBSCO、Web of Science 和 CINAHL 数据库。
纳入标准为(1)接受 DOAC 治疗的 ICH 成年患者(年龄≥18 岁),(2)DOAC 逆转,以及(3)报告安全性和抗凝逆转结果。所有非人类研究和病例报告、需要抗凝逆转或不同 DOAC 逆转剂剂量方案的缺血性卒中患者评估研究,以及 DOAC 和华法林混合研究组均被排除。
使用系统评价和荟萃分析的 Preferred Reporting Items 指南提取数据并评估数据质量和有效性。两名审查员独立选择研究并提取数据。使用随机效应模型汇总数据。
主要结局是抗凝逆转的比例。主要安全性终点是逆转剂后所有原因死亡率和血栓栓塞事件。
共有 36 项研究符合纳入标准,共纳入 1832 例患者(967 例接受 4 因子凝血酶原复合物浓缩物[4F-PCC];525 例接受andexanet alfa [AA];340 例接受idarucizumab)。平均年龄为 76 岁(范围,68-83 岁),57%为男性。对于 4F-PCC,抗凝逆转率为 77%(95%CI,72%-82%;I2=55%);所有原因死亡率为 26%(95%CI,20%-32%;I2=68%),血栓栓塞事件发生率为 8%(95%CI,5%-12%;I2=41%)。对于 AA,抗凝逆转率为 75%(95%CI,67%-81%;I2=48%);所有原因死亡率为 24%(95%CI,16%-34%;I2=73%),血栓栓塞事件发生率为 14%(95%CI,10%-19%;I2=16%)。idarucizumab 逆转 dabigatran 的抗凝逆转率为 82%(95%CI,55%-95%;I2=41%),所有原因死亡率为 11%(95%CI,8%-15%;I2=0%),血栓栓塞事件发生率为 5%(95%CI,3%-8%;I2=0%)。4F-PCC 和 AA 的直接回顾性比较显示,在抗凝逆转、比例死亡率或血栓栓塞事件方面没有差异。
在没有随机临床试验比较的情况下,本系统评价和荟萃分析中 DOAC 逆转剂在管理 ICH 方面的总体抗凝逆转、死亡率和血栓栓塞事件发生率似乎相似。成本、机构配方状态和可及性可能会限制逆转剂的选择,特别是在小型社区医院。