Moula Amalia I, Romeo Jamie L R, Parise Gianmarco, Parise Orlando, Maessen Jos G, Natour Ehsan, Bidar Elham, Gelsomino Sandro
Cardiovascular Center, CARIM School for Cardiovascular Disease, University Hospital Maastricht, University of Maastricht, Maastricht, Netherlands.
Front Cardiovasc Med. 2022 Oct 20;9:999314. doi: 10.3389/fcvm.2022.999314. eCollection 2022.
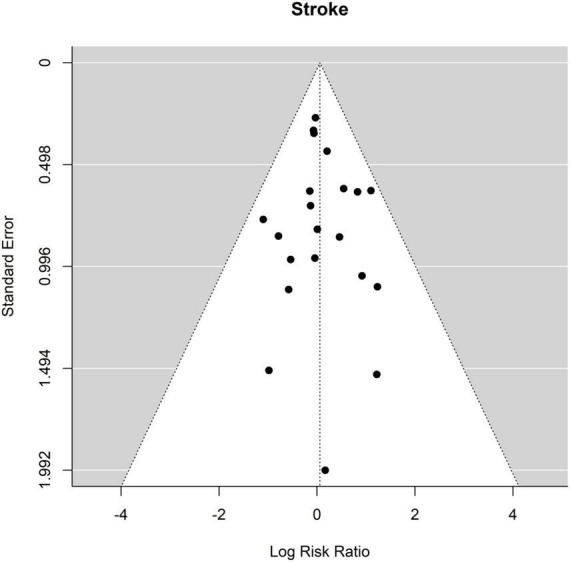
Treatment of aortic arch aneurysms and dissections require highly complex surgical procedures with devastating complications and mortality rates. Currently, repair of the complete arch until the proximal descending thoracic aorta consists of a two-stage procedure, called elephant trunk (ET) technique, or a single stage a single-stage technique referred to as frozen elephant trunk (FET). There is conflicting evidence about the perioperative results of ET in comparison with FET. We carried out a meta-analysis to investigate possible differences in perioperative and early (up to 30 days) outcomes of ET vs. FET, particularly for mortality, spinal cord injury (SCI), stroke, and renal failure. We also performed a meta-regression to explore the effects of age and sex as possible cofactors. Twenty-one studies containing data from interventions conducted between 1997 and 2019 and published between 2008 and 2021 with 3153 patients (68.5% male) were included. ET was applied to 1,693 patients (53.7%) and FET to 1460 (46.3%). Overall mortality after ET was 250/1693 (14.8%) and after FET 116/1460 (7.9%). Relative risk (RR) and 95% confidence interval (CI) were 1.37 [1.04 to 1.81], = 0.027. There was no significant effect of age and sex. SCI occurrence after the second stage of ET was 45/1693 (2.7%) and after FET 70/1,460 patients (4.8%) RR 0.53 [0.35 to 0.81], = 0.004. Age and sex were not associated with the risk of SCI. No significant differences were observed between ET and FET in the incidence of stroke and renal failure. Our results indicate that ET is associated with higher early mortality but lower incidence of SCI compared to FET. When studies published in the last 5 years were analyzed, no significant differences in mortality or SCI were found between ET and FET. This difference is attributed to a decrease in mortality after ET, as the mortality after FET did not change significantly over time.
主动脉弓动脉瘤和夹层的治疗需要高度复杂的外科手术,且伴有严重的并发症和死亡率。目前,修复整个主动脉弓直至胸降主动脉近端包括一种两阶段手术,称为象鼻术(ET),或一种单阶段技术,称为冰冻象鼻术(FET)。关于ET与FET围手术期结果的证据存在矛盾。我们进行了一项荟萃分析,以研究ET与FET围手术期及早期(至30天)结果的可能差异,特别是在死亡率、脊髓损伤(SCI)、中风和肾衰竭方面。我们还进行了荟萃回归分析,以探讨年龄和性别作为可能的协变量的影响。纳入了21项研究,这些研究包含1997年至2019年间进行干预的数据,并于2008年至2021年间发表,共3153例患者(68.5%为男性)。1693例患者(53.7%)采用ET治疗,1460例患者(46.3%)采用FET治疗。ET术后总体死亡率为250/1693(14.8%),FET术后为116/1460(7.9%)。相对风险(RR)和95%置信区间(CI)为1.37 [1.04至1.81],P = 0.027。年龄和性别无显著影响。ET第二阶段术后SCI发生率为45/1693(2.7%),FET术后为70/1460例患者(4.8%),RR 0.53 [0.35至0.81],P = 0.004。年龄和性别与SCI风险无关。ET和FET在中风和肾衰竭发生率方面未观察到显著差异。我们的结果表明,与FET相比,ET与更高的早期死亡率相关,但SCI发生率更低。当分析过去5年发表的研究时,ET和FET在死亡率或SCI方面未发现显著差异。这种差异归因于ET术后死亡率的降低,因为FET术后死亡率随时间没有显著变化。