Ngiam Jinghao Nicholas, Chew Nicholas W S, Pramotedham Thanawin, Tan Benjamin Yong-Qiang, Sia Ching-Hui, Loh Poay Huan, Ruan Wen, Tay Edgar, Kong William K F, Yeo Tiong-Cheng, Poh Kian-Keong
Department of Medicine, National University Health System, Singapore.
Department of Cardiology, National University Heart Centre Singapore, National University Health System, Singapore.
JACC Asia. 2021 Jun 15;1(1):105-111. doi: 10.1016/j.jacasi.2021.05.004. eCollection 2021 Jun.
Aortic regurgitation (AR) is a common comorbidity in patients with aortic stenosis (AS), but coexisting AR has often been excluded from major clinical studies on AS. The impact of coexisting AR on the natural history of AS has not been well-described.
The authors compared clinical outcomes in medically managed patients with moderate-to-severe AS with or without coexisting AR.
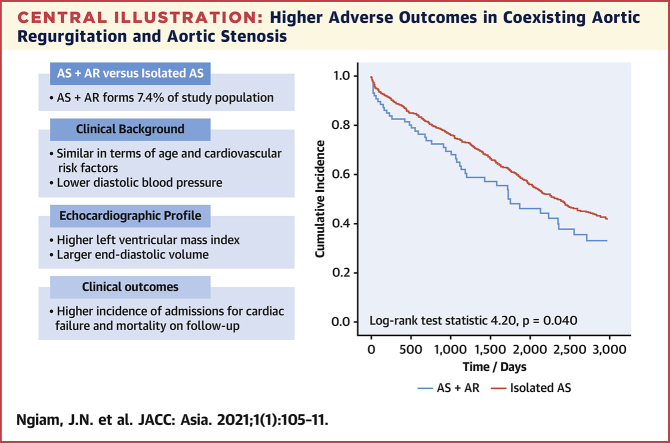
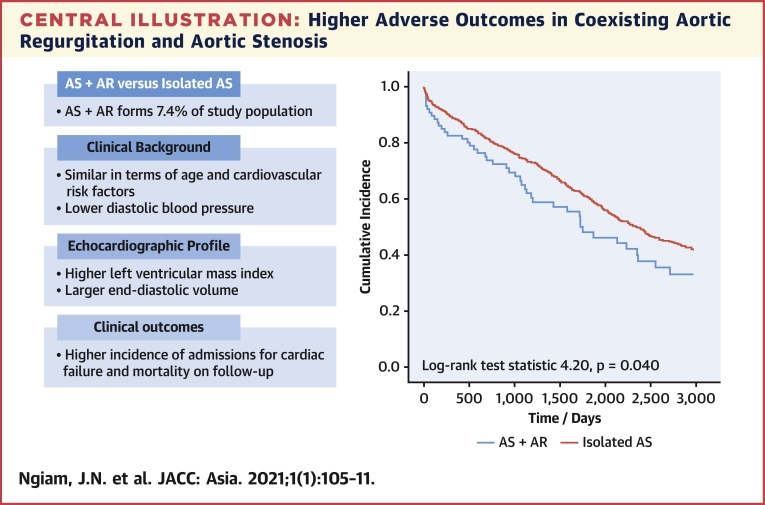
Consecutive patients (N = 1,188) with index echocardiographic diagnosis of moderate-to-severe AS (aortic valve area <1.5 cm) were studied. All patients were medically managed and were divided into those with coexisting AR (at least moderate severity) and those without. Adverse composite clinical outcomes were defined as mortality or admissions for congestive cardiac failure on subsequent follow-up. The authors compared differences in clinical profile and outcomes between the groups.
There were 88 patients (7.4%) with coexisting AR and AS. These patients did not differ significantly in age, but had lower body mass index (22.9 ± 3.8 vs 25.3 ± 5.1 kg/m), lower diastolic blood pressure (68.7 ± 10.7 vs 72.2 ± 12.3 mm Hg), larger end-diastolic volume index (68.8 ± 18.8 vs 60.4 ± 17.8 mL/m) and larger left ventricular mass index (118.6 ± 36.4 vs 108.9 ± 33.1 g/m). The prevalence of cardiovascular risk factors did not differ significantly. Coexisting AR was associated with increased incidence of adverse outcomes (log-rank 4.20; = 0.040). On multivariable Cox regression, coexisting AR remained independently associated with adverse outcomes (HR: 1.36; 95% CI: 1.02-1.82) after adjusting for age, AS severity, left ventricular ejection fraction, and year of study.
In patients with AS, coexisting AR was associated with changes in echocardiographic profile and adverse outcomes.
主动脉瓣反流(AR)是主动脉瓣狭窄(AS)患者常见的合并症,但并存的AR在关于AS的主要临床研究中常常被排除。并存的AR对AS自然病程的影响尚未得到充分描述。
作者比较了接受药物治疗的中重度AS患者并存或不并存AR时的临床结局。
对连续入选的1188例经超声心动图首次诊断为中重度AS(主动脉瓣面积<1.5cm²)的患者进行研究。所有患者均接受药物治疗,并分为并存AR(至少中度严重程度)组和不并存AR组。不良复合临床结局定义为后续随访期间的死亡或因充血性心力衰竭住院。作者比较了两组之间临床特征和结局的差异。
有88例(7.4%)患者并存AR和AS。这些患者在年龄上无显著差异,但体重指数较低(22.9±3.8 vs 25.3±5.1kg/m²),舒张压较低(68.7±10.7 vs 72.2±12.3mmHg),舒张末期容积指数较大(68.8±18.8 vs 60.4±17.8mL/m²),左心室质量指数较大(118.6±36.4 vs 108.9±33.1g/m²)。心血管危险因素的患病率无显著差异。并存AR与不良结局发生率增加相关(对数秩检验χ²=4.20;P=0.040)。在多变量Cox回归分析中,在调整年龄、AS严重程度、左心室射血分数和研究年份后,并存AR仍与不良结局独立相关(HR:1.36;95%CI:1.02-1.82)。
在AS患者中,并存AR与超声心动图特征改变及不良结局相关。