Tarakji Khaldoun G, Korantzopoulos Panagiotis, Philippon Francois, Biffi Mauro, Mittal Suneet, Poole Jeanne E, Kennergren Charles, Lexcen Daniel R, Lande Jeff D, Hilleren Gregory, Seshadri Swathi, Wilkoff Bruce L
Department of Cardiovascular Medicine, Cleveland Clinic, Cleveland, Ohio.
First Department of Cardiology, University Hospital of Ioannina, Ioannina, Greece.
Heart Rhythm O2. 2022 Jun 16;3(5):466-473. doi: 10.1016/j.hroo.2022.05.012. eCollection 2022 Oct.
Implant site hematoma is a known complication of cardiac device procedures and can lead to major consequences.
To evaluate risk factors for hematoma and further understand the relationship between anticoagulant (AC), antiplatelet (AP) use, and hematoma development.
We included 6800 patients from the WRAP-IT trial. To assess baseline and procedural characteristics associated with hematoma within the first 30 days postprocedure, a stepwise Cox regression model was implemented with minimal Akaike information criterion. Cox regressions were also used to evaluate AC/AP use and hematoma risk.
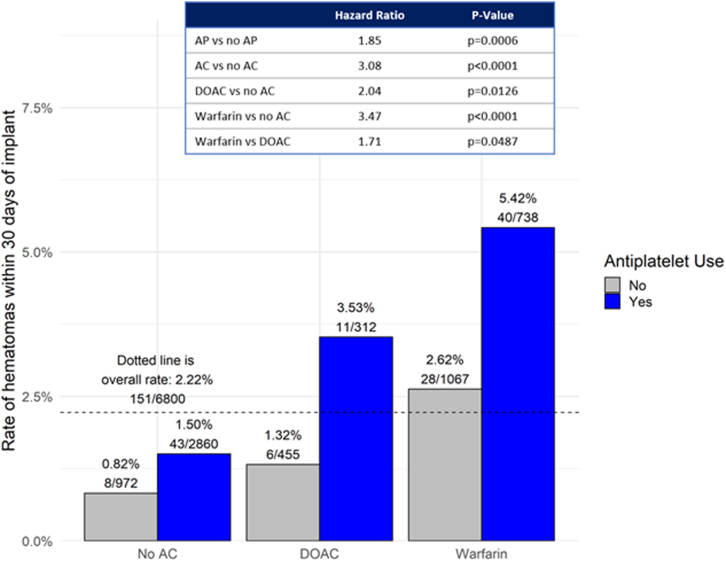
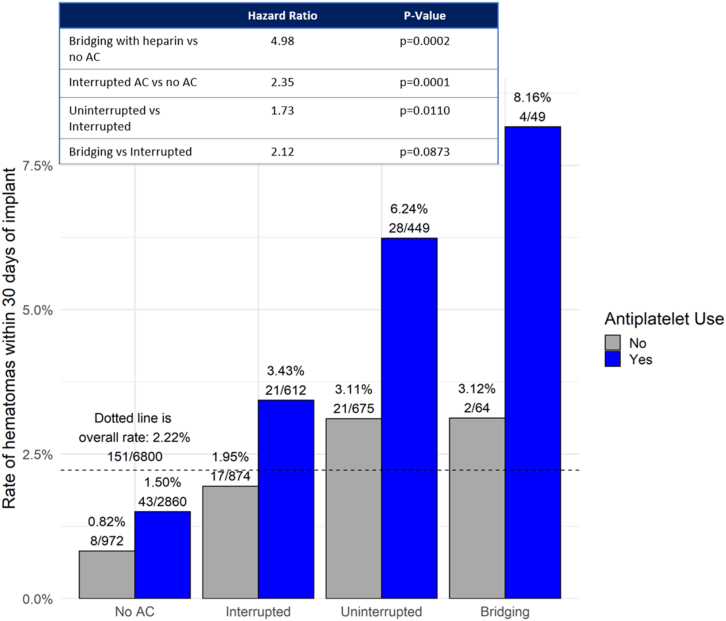
The overall rate of hematoma was 2.2%. The model identified 11 baseline and procedural characteristics associated with hematoma risk. AC use (hazard ratio [HR]: 2.44, < .001), lower body mass index (HR: 1.06, < .001), and history of valve surgery (HR: 2.11, < .001) were associated with the highest risk. AP use, male sex, history of coronary artery disease, existing pocket, history of nonischemic cardiomyopathy, number of previous cardiac implantable electronic device (CIED) procedures, procedure time, and lead revision were associated with moderate risk. Antithrombotic use was high overall (86%) and AC+AP use was highly predictive of hematoma risk. Regardless of AC status, AP use was associated with an almost doubling of risk vs no AP (HR = 1.85, = .0006) in the general cohort. Interruption of AC was associated with the lowest hematoma risk (HR = 2.35) while heparin bridging (HR = 4.98) and AP use vs no AP use (HR = 1.85) was associated with the highest hematoma risk.
The results of this analysis highlight risk factors associated with the development of hematoma in patients undergoing CIED procedures and can inform antithrombotic management.
植入部位血肿是心脏设备手术已知的并发症,可导致严重后果。
评估血肿的危险因素,并进一步了解抗凝剂(AC)、抗血小板药物(AP)的使用与血肿形成之间的关系。
我们纳入了WRAP-IT试验中的6800例患者。为了评估术后30天内与血肿相关的基线和手术特征,采用了具有最小赤池信息准则的逐步Cox回归模型。Cox回归也用于评估AC/AP的使用和血肿风险。
血肿的总体发生率为2.2%。该模型确定了11个与血肿风险相关的基线和手术特征。使用AC(风险比[HR]:2.44,P<0.001)、较低的体重指数(HR:1.06,P<0.001)和瓣膜手术史(HR:2.11,P<0.001)与最高风险相关。使用AP、男性、冠状动脉疾病史、现有囊袋、非缺血性心肌病病史、既往心脏植入式电子设备(CIED)手术次数、手术时间和导线翻修与中度风险相关。总体抗栓药物使用率较高(86%),AC+AP联合使用对血肿风险具有高度预测性。在总体队列中,无论AC状态如何,使用AP与未使用AP相比,风险几乎增加一倍(HR = 1.85,P = 0.0006)。中断AC与最低的血肿风险相关(HR = 2.35),而肝素桥接(HR = 4.98)和使用AP与未使用AP(HR = 1.85)与最高的血肿风险相关。
该分析结果突出显示了接受CIED手术患者发生血肿的相关危险因素,并可为抗栓治疗管理提供参考。