Kusano Kengo, Ishibashi Kohei, Noda Takashi, Nakajima Kenzaburo, Nakasuka Kosuke, Terasaki Satoshi, Hattori Yusuke, Nagayama Tomomi, Mori Kazuki, Takaya Yoichi, Miyamoto Koji, Nagase Satoshi, Aiba Takeshi, Yasuda Satoshi, Kitakaze Masafumi, Kamakura Shiro, Yazaki Yoshikazu, Morimoto Shin-Ichiro, Isobe Mitsuaki, Terasaki Fumio
Department of Cardiovascular Medicine, National Cerebral and Cardiovascular Center, Osaka, Japan.
Department of Cardio-Renal Medicine and Hypertension, Nagoya City University, Nagoya, Japan.
JACC Asia. 2021 Dec 7;1(3):385-395. doi: 10.1016/j.jacasi.2021.09.005. eCollection 2021 Dec.
Diagnosis of cardiac sarcoidosis (CS) is sometimes difficult due to a low positive rate of epithelioid granulomas by endomyocardial biopsy (EMB). Accordingly, Japanese guidelines can allow the CS diagnosis using clinical data alone without EMB results (clinical CS) since 2006. However, little is known about prognosis and outcome of clinical CS.
Purpose of this study was to analyze the prognosis, outcomes, and response to corticosteroid of clinical CS using large-scale cohort survey.
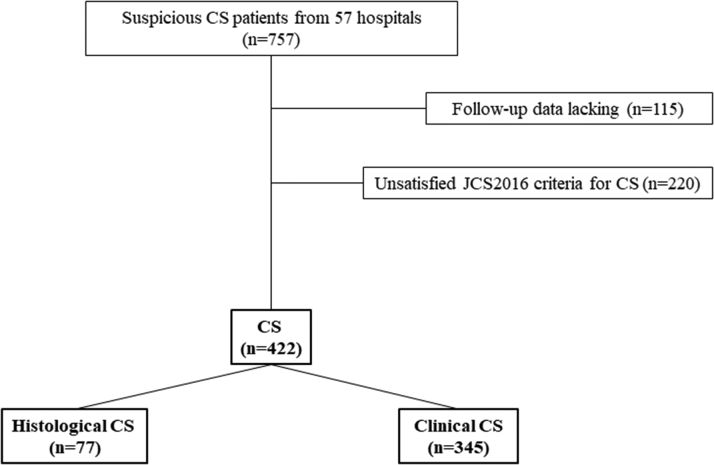
Overall, 422 CS patients (mean age 60 ± 13 years, 68% female, median follow-up period of 5 years), including 345 clinical CS and 77 EMB-positive patients, histologically diagnosed CS (histological CS) by Japanese guidelines, were enrolled and examined.
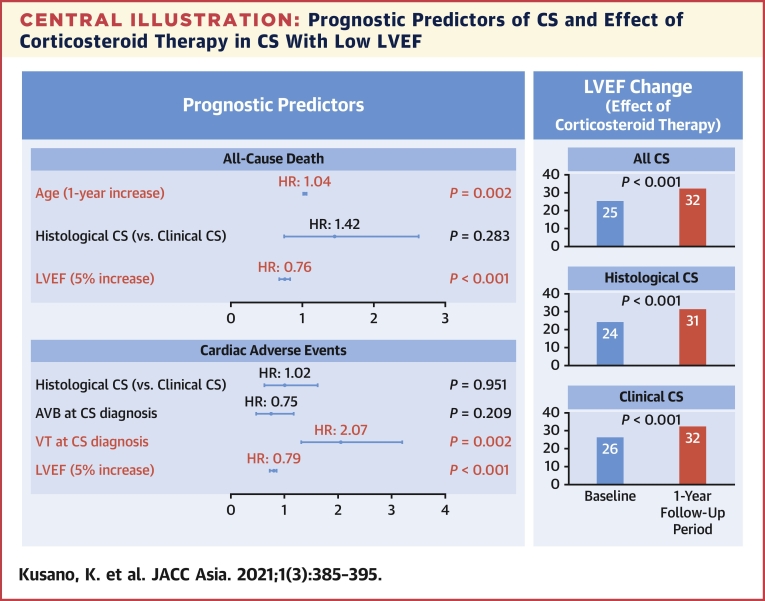
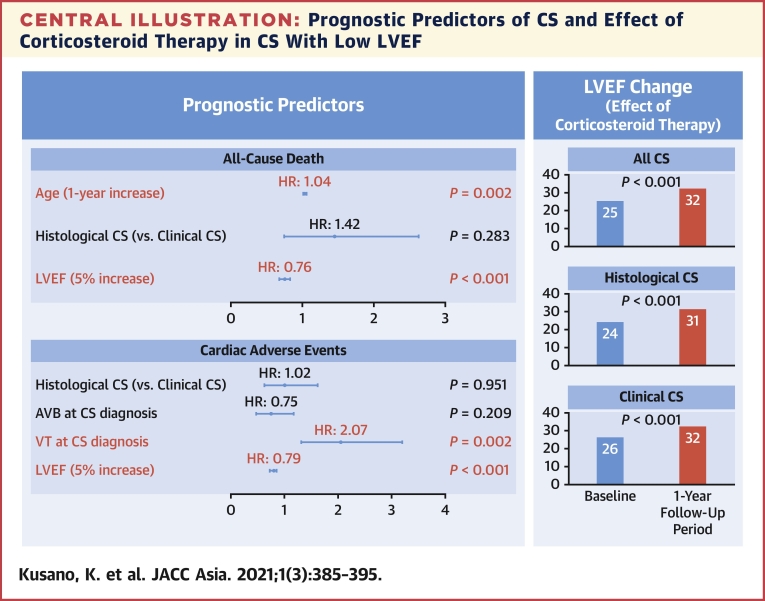
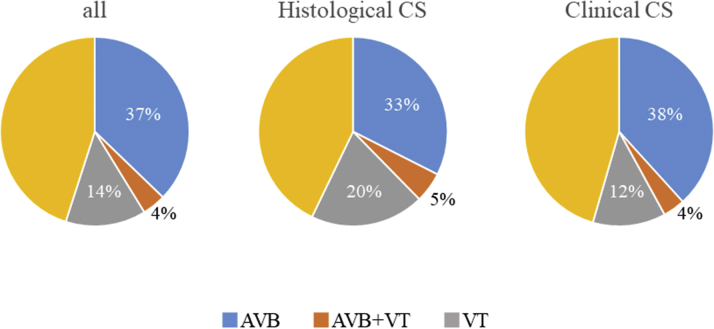
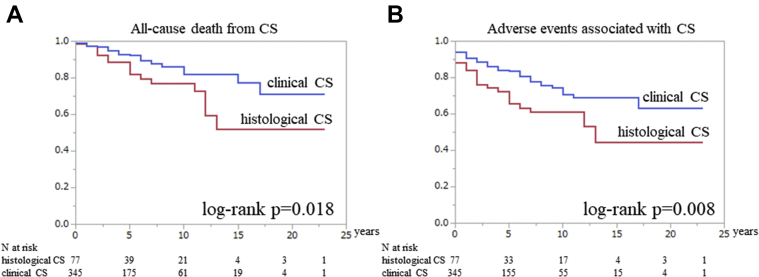
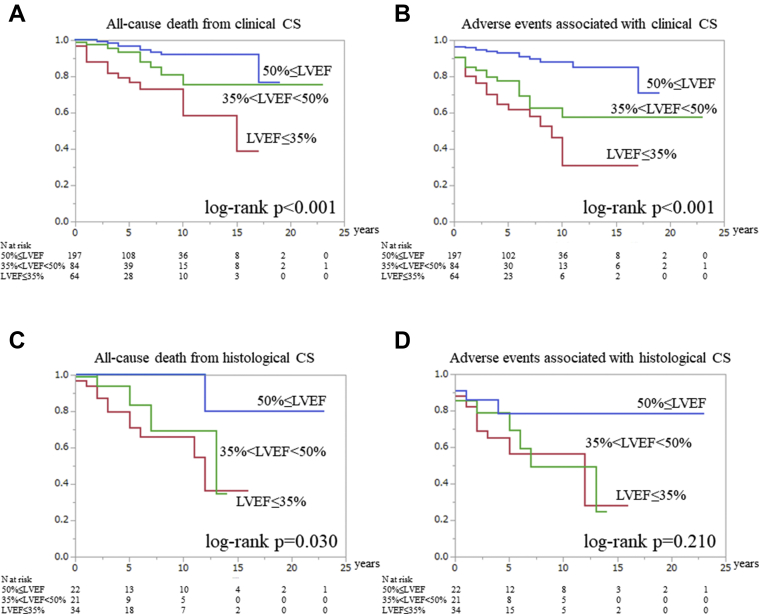
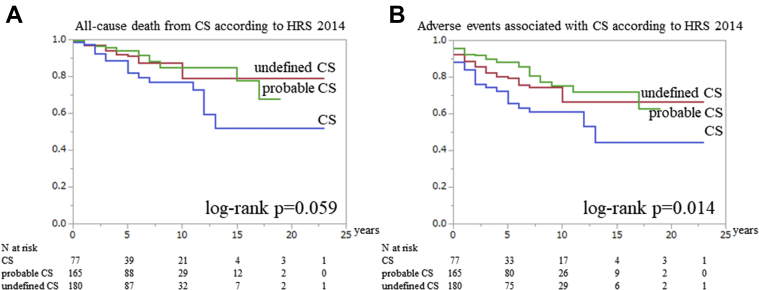
Clinical profile (age, sex, initial cardiac arrhythmias, and abnormal uptake of gallium-67 scintigraphy or F-fluorodeoxyglucose positron emission tomography in heart) was similar in both groups. Although clinical CS had better prognosis ( 0.018) and outcome (all-cause death, appropriate defibrillator therapy, and heart transplantation; 0.008), multivariate Cox hazard analysis revealed that left ventricular ejection fraction (LVEF) and sustained ventricular tachycardia history were independently associated with outcome ( 0.001 and 0.002, respectively), but not with the diagnosed CS category. Moreover, similar LVEF recovery after corticosteroid was observed in both groups with low LVEF (≤35%) at the 1-year follow-up period ( 0.001).
In clinical CS according to the Japanese guideline, prophylactic implantable-cardioverter-defibrillator and immunosuppressive therapy are important in patients with low LVEF or ventricular tachycardia history, similar to histological CS.
由于心内膜心肌活检(EMB)中上皮样肉芽肿的阳性率较低,心脏结节病(CS)的诊断有时较为困难。因此,自2006年起,日本指南允许在无EMB结果的情况下仅使用临床数据进行CS诊断(临床CS)。然而,关于临床CS的预后和结局知之甚少。
本研究旨在通过大规模队列调查分析临床CS的预后、结局及对皮质类固醇的反应。
总共纳入并检查了422例CS患者(平均年龄60±13岁,68%为女性,中位随访期5年),其中包括345例临床CS患者和77例EMB阳性患者,这些患者根据日本指南经组织学诊断为CS(组织学CS)。
两组的临床特征(年龄、性别、初始心律失常以及心脏镓-67闪烁显像或F-氟脱氧葡萄糖正电子发射断层显像异常摄取)相似。尽管临床CS的预后较好(P=0.018)且结局较好(全因死亡、适当的除颤器治疗和心脏移植;P=0.008),但多因素Cox风险分析显示,左心室射血分数(LVEF)和持续性室性心动过速病史与结局独立相关(分别为P=0.001和P=0.002),而与诊断的CS类别无关。此外,在1年随访期LVEF较低(≤35%)的两组患者中,观察到皮质类固醇治疗后LVEF恢复情况相似(P=0.001)。
在日本指南定义的临床CS中,对于LVEF较低或有室性心动过速病史的患者,预防性植入心脏复律除颤器和免疫抑制治疗与组织学CS患者一样重要。