Department of Nephrology and Organ Transplantation, University Hospital of Toulouse, and French Intensive Care Renal Network, 31000, Toulouse, France.
National Institute of Health and Medical Research (INSERM), UMR 1297, Institute of Cardiovascular and Metabolic Disease, 31000, Toulouse, France.
Crit Care. 2022 Nov 7;26(1):344. doi: 10.1186/s13054-022-04193-9.
The delayed diagnosis of acute kidney injury (AKI) episodes and the lack of specificity of current single AKI biomarkers hamper its management. Urinary peptidome analysis may help to identify early molecular changes in AKI and grasp its complexity to identify potential targetable molecular pathways.
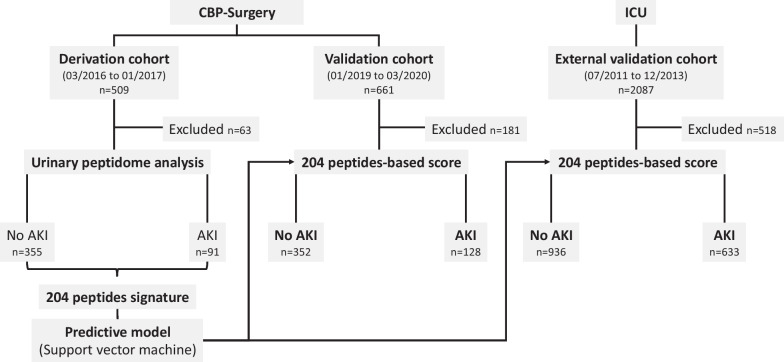
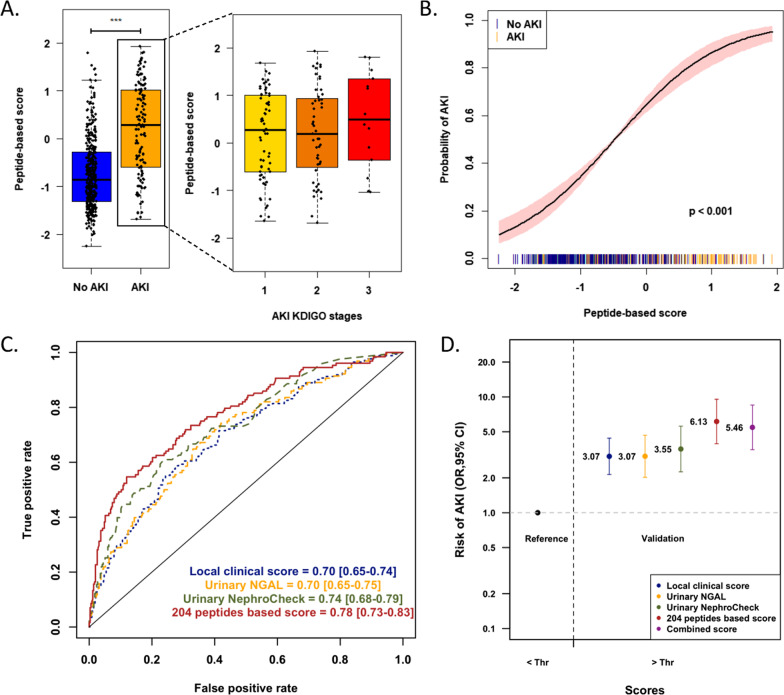
In derivation and validation cohorts totalizing 1170 major cardiac bypass surgery patients and in an external cohort of 1569 intensive care unit (ICU) patients, a peptide-based score predictive of AKI (7-day KDIGO classification) was developed, validated, and compared to the reference biomarker urinary NGAL and NephroCheck and clinical scores.
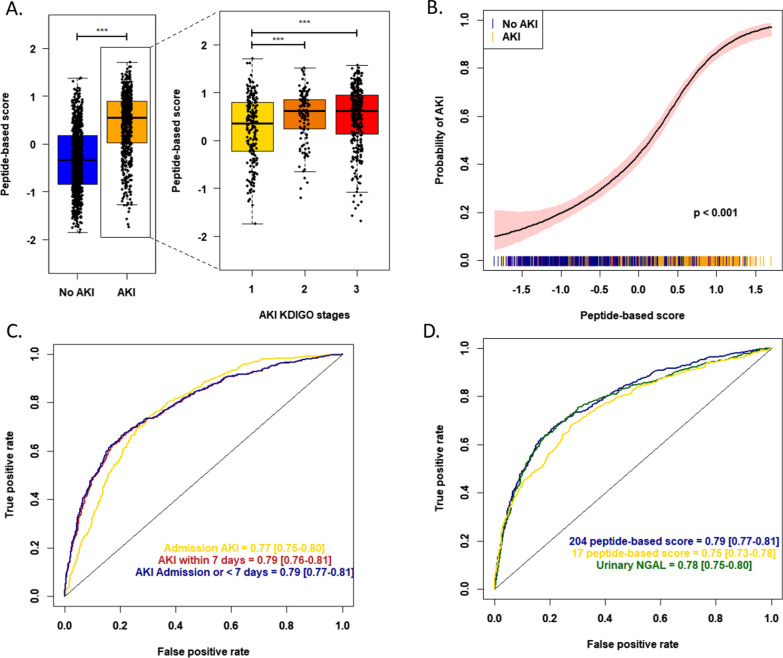
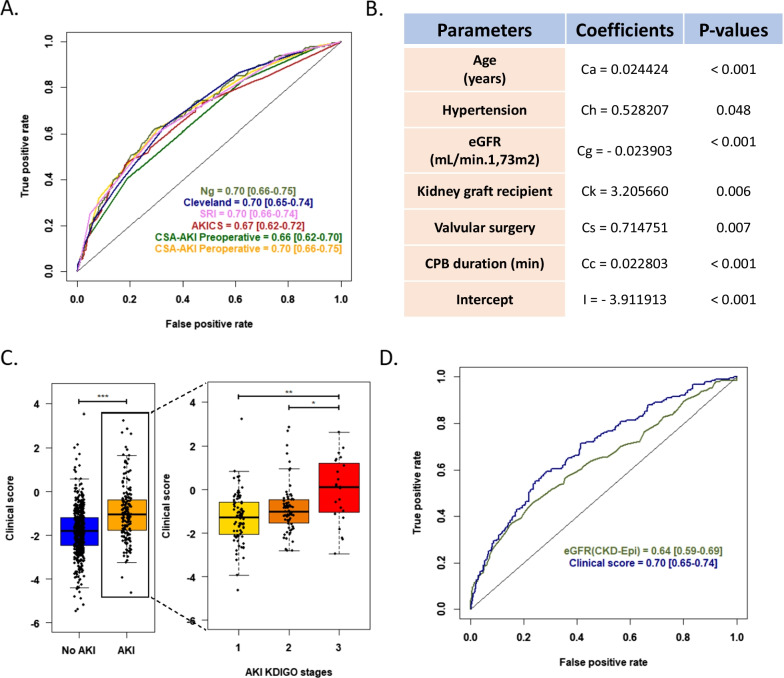
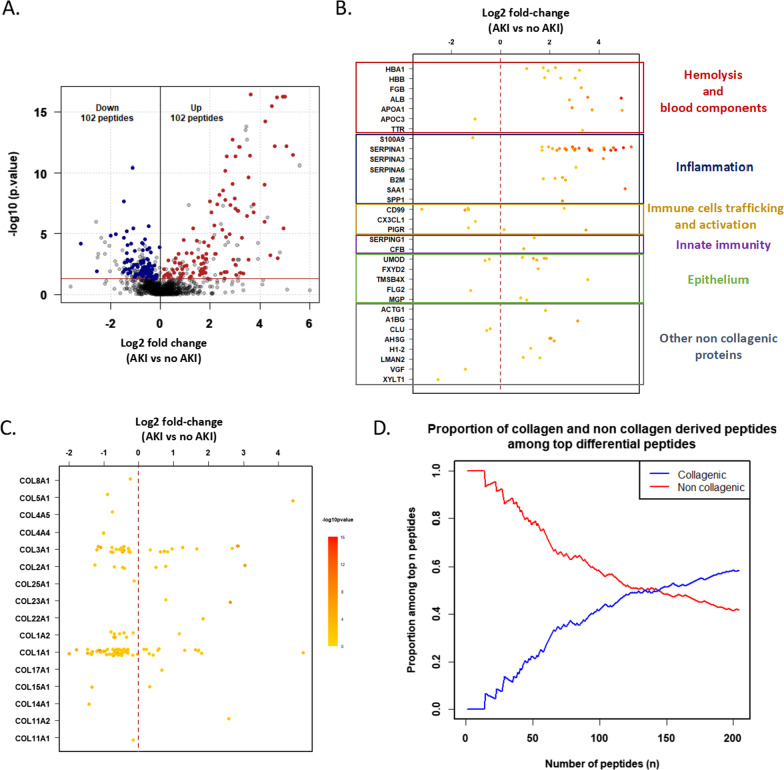
A set of 204 urinary peptides derived from 48 proteins related to hemolysis, inflammation, immune cells trafficking, innate immunity, and cell growth and survival was identified and validated for the early discrimination (< 4 h) of patients according to their risk to develop AKI (OR 6.13 [3.96-9.59], p < 0.001) outperforming reference biomarkers (urinary NGAL and [IGFBP7].[TIMP2] product) and clinical scores. In an external cohort of 1569 ICU patients, performances of the signature were similar (OR 5.92 [4.73-7.45], p < 0.001), and it was also associated with the in-hospital mortality (OR 2.62 [2.05-3.38], p < 0.001).
An overarching AKI physiopathology-driven urinary peptide signature shows significant promise for identifying, at an early stage, patients who will progress to AKI and thus to develop tailored treatments for this frequent and life-threatening condition. Performance of the urine peptide signature is as high as or higher than that of single biomarkers but adds mechanistic information that may help to discriminate sub-phenotypes of AKI offering new therapeutic avenues.
急性肾损伤(AKI)发作的延迟诊断和当前单一 AKI 生物标志物的缺乏特异性,阻碍了其管理。尿肽组分析可能有助于识别 AKI 的早期分子变化,并把握其复杂性,以确定潜在的可靶向分子途径。
在包含 1170 名主要心脏搭桥手术患者的推导和验证队列中,以及在包含 1569 名重症监护病房(ICU)患者的外部队列中,开发、验证了一种基于肽的 AKI 预测评分(7 天 KDIGO 分类),并将其与参考生物标志物尿 NGAL 和 NephroCheck 以及临床评分进行比较。
从与溶血、炎症、免疫细胞迁移、固有免疫以及细胞生长和存活相关的 48 种蛋白质中鉴定和验证了一组 204 种尿肽,用于根据患者发生 AKI 的风险(OR 6.13 [3.96-9.59],p < 0.001)进行早期(<4 小时)区分,优于参考生物标志物(尿 NGAL 和 [IGFBP7].[TIMP2] 产物)和临床评分。在包含 1569 名 ICU 患者的外部队列中,该特征的表现相似(OR 5.92 [4.73-7.45],p < 0.001),并且与住院死亡率相关(OR 2.62 [2.05-3.38],p < 0.001)。
一个总体的 AKI 病理生理学驱动的尿肽特征显示出有希望的前景,可以在早期识别出将进展为 AKI 从而需要针对这种常见且危及生命的疾病进行个体化治疗的患者。尿液肽特征的性能与单一生物标志物一样高,甚至更高,但增加了有助于区分 AKI 亚表型的机制信息,为新的治疗途径提供了可能。