Department of Health, Medicine and Caring Sciences, Linköping University, SE-581 83 Linköping, Sweden.
Department of Medicine Huddinge, Karolinska Institutet Karolinska University Hospital, SE-141 86 Stockholm, Sweden.
Eur Heart J. 2023 Jan 14;44(3):196-204. doi: 10.1093/eurheartj/ehac547.
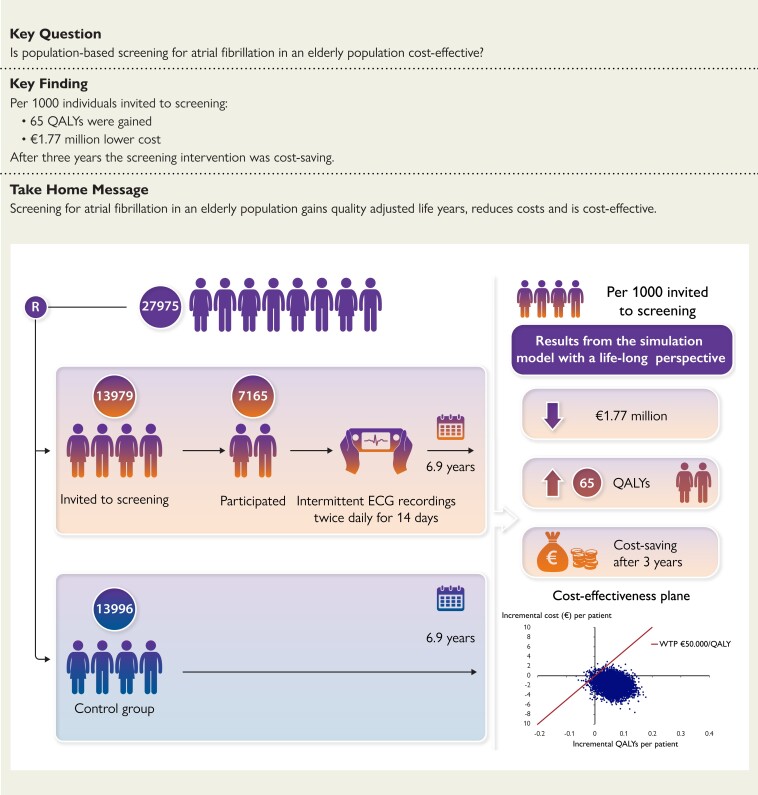
Previous studies on the cost-effectiveness of screening for atrial fibrillation (AF) are based on assumptions of long-term clinical effects. The STROKESTOP study, which randomised 27 975 persons aged 75/76 years into a screening invitation group and a control group, has a median follow-up time of 6.9 years. The aim of this study was to estimate the cost-effectiveness of population-based screening for AF using clinical outcomes.
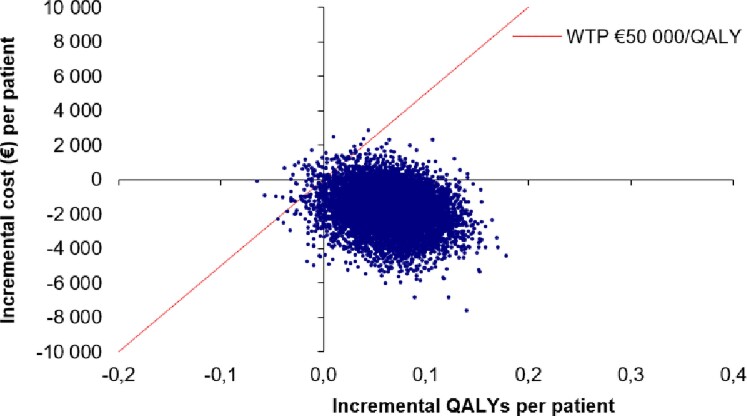
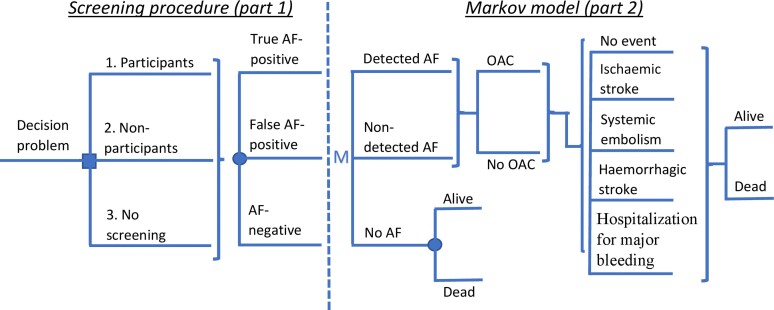
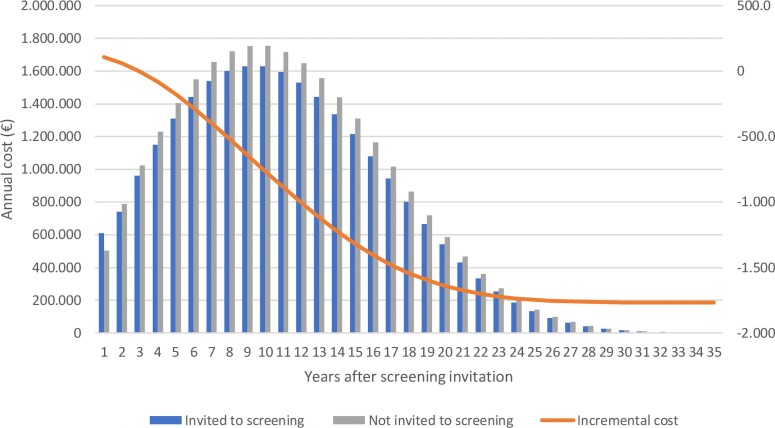
The analysis is based on a Markov cohort model. The prevalence of AF, the use of oral anticoagulation, clinical event data, and all-cause mortality were taken from the STROKESTOP study. The cost for clinical events, age-specific utilities, utility decrement due to stroke, and stroke death was taken from the literature. Uncertainty in the model was considered in a probabilistic sensitivity analysis. Per 1000 individuals invited to the screening, there were 77 gained life years and 65 gained quality-adjusted life years. The incremental cost was €1.77 million lower in the screening invitation group. Gained quality-adjusted life years to a lower cost means that the screening strategy was dominant. The result from 10 000 Monte Carlo simulations showed that the AF screening strategy was cost-effective in 99.2% and cost-saving in 92.7% of the simulations. In the base-case scenario, screening of 1000 individuals resulted in 10.6 [95% confidence interval (CI): -22.5 to 1.4] fewer strokes (8.4 ischaemic and 2.2 haemorrhagic strokes), 1.0 (95% CI: -1.9 to 4.1) more cases of systemic embolism, and 2.9 (95% CI: -18.2 to 13.1) fewer bleedings associated with hospitalization.
Based on the STROKESTOP study, this analysis shows that a broad AF screening strategy in an elderly population is cost-effective. Efforts should be made to increase screening participation.
先前关于心房颤动(AF)筛查的成本效益研究是基于对长期临床效果的假设。STROKESTOP 研究将 27975 名 75/76 岁的患者随机分为筛查邀请组和对照组,中位随访时间为 6.9 年。本研究旨在使用临床结局来估计基于人群的 AF 筛查的成本效益。
该分析基于马尔可夫队列模型。AF 的患病率、口服抗凝药物的使用、临床事件数据和全因死亡率均来自 STROKESTOP 研究。临床事件、年龄特定效用、因中风导致的效用下降和中风死亡的费用均来自文献。在概率敏感性分析中考虑了模型中的不确定性。每邀请 1000 人进行筛查,可获得 77 个生存年和 65 个质量调整生存年。筛查邀请组的增量成本低 177 万欧元。以更低的成本获得更多的质量调整生存年意味着筛查策略具有优势。来自 10000 次蒙特卡罗模拟的结果表明,在 99.2%的模拟中,AF 筛查策略具有成本效益,在 92.7%的模拟中具有成本节约。在基本情况下,对 1000 人进行筛查可减少 10.6 [95%置信区间(CI):-22.5 至 1.4]例中风(8.4 例缺血性和 2.2 例出血性中风)、1.0(95%CI:-1.9 至 4.1)例全身性栓塞和 2.9(95%CI:-18.2 至 13.1)例与住院相关的出血。
基于 STROKESTOP 研究,本分析表明,在老年人群中广泛开展 AF 筛查具有成本效益。应努力提高筛查参与率。