Popescu Alexandru Dan, Carsote Mara, Valea Ana, Nicola Andreea Gabriela, Dascălu Ionela Teodora, Tircă Tiberiu, Abdul-Razzak Jaqueline, Țuculină Mihaela Jana
Department of Endodontics, Faculty of Dental Medicine, University of Medicine and Pharmacy of Craiova, 200349 Craiova, Romania.
Department of Endocrinology, Carol Davila University of Medicine and Pharmacy & C.I. Parhon National Institute of Endocrinology, 011683 Bucharest, Romania.
Diagnostics (Basel). 2022 Nov 2;12(11):2669. doi: 10.3390/diagnostics12112669.
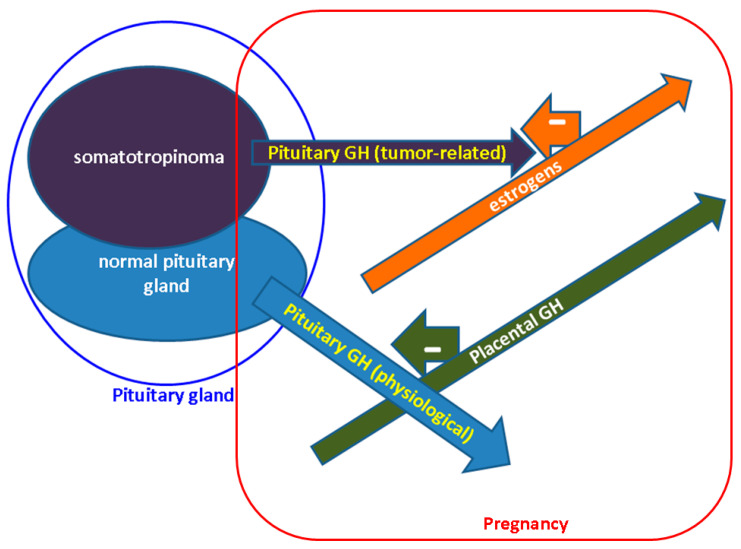
Acromegaly-related sub/infertility, tidily related to suboptimal disease control (1/2 of cases), correlates with hyperprolactinemia (1/3 of patients), hypogonadotropic hypogonadism—mostly affecting the pituitary axis in hypopituitarism (10−80%), and negative effects of glucose profile (GP) anomalies (10−70%); thus, pregnancy is an exceptional event. Placental GH (Growth Hormone) increases from weeks 5−15 with a peak at week 37, stimulating liver IGF1 and inhibiting pituitary GH secreted by normal hypophysis, not by somatotropinoma. However, estrogens induce a GH resistance status, protecting the fetus form GH excess; thus a full-term, healthy pregnancy may be possible. This is a narrative review of acromegaly that approaches cardio-metabolic features (CMFs), somatotropinoma expansion (STE), management adjustment (MNA) and maternal-fetal outcomes (MFOs) during pregnancy. Based on our method (original, in extenso, English—published articles on PubMed, between January 2012 and September 2022), we identified 24 original papers—13 studies (3 to 141 acromegalic pregnancies per study), and 11 single cases reports (a total of 344 pregnancies and an additional prior unpublished report). With respect to maternal acromegaly, pregnancies are spontaneous or due to therapy for infertility (clomiphene, gonadotropins or GnRH) and, lately, assisted reproduction techniques (ARTs); there are no consistent data on pregnancies with paternal acromegaly. CMFs are the most important complications (7.7−50%), especially concerning worsening of HBP (including pre/eclampsia) and GP anomalies, including gestational diabetes mellitus (DM); the best predictor is the level of disease control at conception (IGF1), and, probably, family history of 2DM, and body mass index. STE occurs rarely (a rate of 0 to 9%); some of it symptoms are headache and visual field anomalies; it is treated with somatostatin analogues (SSAs) or alternatively dopamine agonists (DAs); lately, second trimester selective hypophysectomy has been used less, since pharmaco-therapy (PT) has proven safe. MNA: PT that, theoretically, needs to be stopped before conception—continued if there was STE or an inoperable tumor (no clear period of exposure, preferably, only first trimester). Most data are on octreotide > lanreotide, followed by DAs and pegvisomant, and there are none on pasireotide. Further follow-up is required: a prompt postpartum re-assessment of the mother’s disease; we only have a few data confirming the safety of SSAs during lactation and long-term normal growth and developmental of the newborn (a maximum of 15 years). MFO seem similar between PT + ve and PT − ve, regardless of PT duration; the additional risk is actually due to CMF. One study showed a 2-year median between hypophysectomy and pregnancy. Conclusion: Close surveillance of disease burden is required, particularly, concerning CMF; a personalized approach is useful; the level of statistical evidence is expected to expand due to recent progress in MNA and ART.
肢端肥大症相关的生育力低下/不育,与疾病控制不佳密切相关(半数病例),与高催乳素血症(三分之一患者)、低促性腺激素性性腺功能减退(主要影响垂体功能减退患者的垂体轴,发生率为10% - 80%)以及糖代谢异常的负面影响(发生率为10% - 70%)相关;因此,怀孕是罕见事件。胎盘生长激素(GH)在孕5 - 15周时升高,在孕37周时达到峰值,刺激肝脏产生胰岛素样生长因子1(IGF1),并抑制正常垂体而非生长激素瘤分泌的垂体GH。然而,雌激素会诱导GH抵抗状态,保护胎儿免受GH过量影响;因此,有可能实现足月健康妊娠。这是一篇关于肢端肥大症的叙述性综述,探讨了孕期的心脏代谢特征(CMF)、生长激素瘤扩展(STE)、管理调整(MNA)和母胎结局(MFO)。基于我们的方法(原始、详尽、英文——2012年1月至2022年9月在PubMed上发表的文章),我们确定了24篇原始论文——13项研究(每项研究有3至141例肢端肥大症患者怀孕)和11篇单病例报告(共344例怀孕,另有一篇之前未发表的报告)。关于母亲患肢端肥大症的情况,怀孕多为自然受孕或因不育治疗(克罗米芬、促性腺激素或促性腺激素释放激素),近来则是辅助生殖技术(ART);关于父亲患肢端肥大症的怀孕情况,尚无一致数据。CMF是最重要的并发症(发生率为7.7% - 50%),尤其涉及高血压病情恶化(包括先兆子痫/子痫)和糖代谢异常,包括妊娠期糖尿病(DM);最佳预测指标是受孕时的疾病控制水平(IGF1),可能还有2型糖尿病家族史和体重指数。STE很少发生(发生率为0至9%);其一些症状为头痛和视野异常;治疗方法为使用生长抑素类似物(SSA)或多巴胺激动剂(DA);近来,由于药物治疗(PT)已被证明安全,孕中期选择性垂体切除术的使用较少。MNA:理论上,PT在受孕前需停用——如果存在STE或肿瘤无法手术切除则继续使用(无明确暴露期,最好仅在孕早期)。大多数数据涉及奥曲肽>兰瑞肽,其次是DA和培维索孟,关于帕西瑞肽则无相关数据。需要进一步随访:产后及时对母亲的疾病进行重新评估;我们仅有少数数据证实SSA在哺乳期的安全性以及新生儿的长期正常生长发育情况(最长15年)。无论PT持续时间如何,PT阳性和PT阴性患者的MFO似乎相似;额外风险实际上是由CMF导致的。一项研究显示垂体切除术后与怀孕的中位间隔时间为两年。结论:需要密切监测疾病负担,尤其是CMF;个性化方法很有用;由于MNA和ART的近期进展,统计证据水平有望提高。