ICMR-Regional Medical Research Centre, Chandrasekharpur, Bhubaneswar, 751023, Odisha, India.
School of Biotechnology, KIIT University, Bhubaneswar, 751024, Odisha, India.
Malar J. 2022 Nov 16;21(1):340. doi: 10.1186/s12936-022-04358-5.
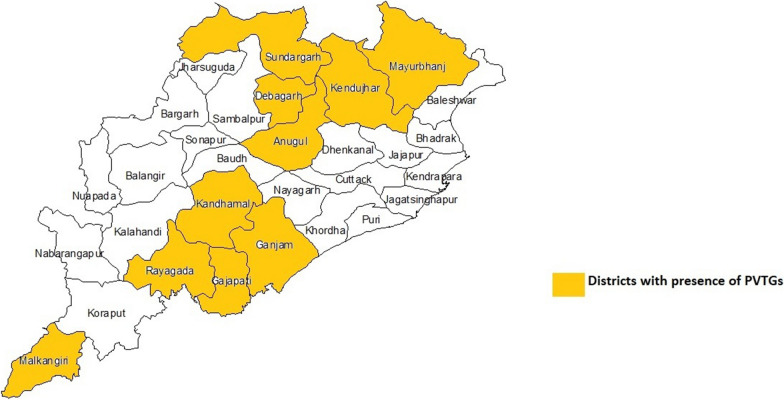
Haemoglobinopathies and G6PD deficiency are inherited disorders found mostly in malaria-endemic areas among different tribal groups of India. However, epidemiological data specific to Particularly Vulnerable Tribal Groups (PVTGs), important for planning and implementing malaria programmes, is limited. Therefore, the present community-based study aimed to assess the prevalence of haemoglobinopathies and G6PD deficiency among the 13 PVTGs found in the state of Odisha, reporting the maximum malaria cases in the country.
This cross-sectional study was conducted from July 2018 to February 2019 in 12 districts, home to all 13 PVTGs, in an estimated sample size of 1461, selected two-stage sampling method. Detection of haemoglobinopathies was done by the variant analyser. Screening of G6PD deficiency was carried out using DPIP method followed by quantification using spectrophotometry. The PCR-RFLP technology was used to determine variant of G6PD deficiency and haplotype analysis of sickle cell, while ARMS-PCR and GAP-PCR was used for detecting the mutation pattern in β-thalassaemia and α-thalassaemia respectively. The diagnosis of malaria was done by Pf-PAN RDT as point of care, followed by nPCR for confirmation and Plasmodium species identification.
The prevalence of sickle cell heterozygotes (AS) was 3.4%, sickle cell homozygous (SS) 0.1%, β-thalassaemia heterozygotes 0.3%, HbS/β-thalassaemia compound heterozygote 0.07%, HbS-α-thalassaemia 2.1%, G6PD deficiency 3.2% and malaria 8.1%. Molecular characterization of β revealed the presence of Arab-Indian haplotype in all HbS cases and IVS 1-5 G → C mutation in all β-thalassaemia cases. In case of α-thal, αα/α-3.7 gene deletion was most frequent (38%), followed by αα/α-4.2 (18%) and α-3.7/α-3.7 (4%). The frequency of G6PD Orissa (131C → G) mutation was found to be 97.9% and G6PD Mediterranean (563C → T) 2.1%. Around 57.4% of G6PD deficient individuals and 16% of the AS were found to be malaria positive.
The present study reveals wide spread prevalence of sickle cell anaemia, α-thalassaemia, G6PD deficiency and malaria in the studied population. Moderate to high prevalence of G6PD deficiency and malaria warrants G6PD testing before treating with primaquine (PQ) for radical cure of Plasmodium vivax. Screening and counselling for HbS is required for the PVTGs of Odisha.
血红蛋白病和葡萄糖-6-磷酸脱氢酶(G6PD)缺乏症是遗传性疾病,主要在印度不同部落群体的疟疾流行地区发现。然而,针对特别脆弱部落群体(PVTGs)的流行病学数据对于规划和实施疟疾项目非常重要,但目前此类数据有限。因此,本社区为基础的研究旨在评估在印度奥里萨邦发现的 13 个 PVTG 中血红蛋白病和 G6PD 缺乏症的流行情况,该邦是全国疟疾病例最多的邦。
这是一项横断面研究,于 2018 年 7 月至 2019 年 2 月在奥里萨邦的 12 个地区进行,这些地区居住着所有 13 个 PVTG,样本量估计为 1461 人,采用两阶段抽样方法选择。血红蛋白病的检测采用变异分析仪进行。使用 DPIP 方法进行 G6PD 缺乏症的筛查,然后使用分光光度法进行定量。PCR-RFLP 技术用于确定 G6PD 缺乏症的变体和镰状细胞的单倍型分析,而 ARMS-PCR 和 GAP-PCR 用于检测β-地中海贫血和α-地中海贫血的突变模式。采用 Pf-PAN RDT 进行疟疾即时检测(POC),随后进行 nPCR 确认和疟原虫种鉴定。
镰状细胞杂合子(AS)的患病率为 3.4%,镰状细胞纯合子(SS)为 0.1%,β-地中海贫血杂合子为 0.3%,HbS/β-地中海贫血复合杂合子为 0.07%,HbS-α-地中海贫血为 2.1%,G6PD 缺乏症为 3.2%,疟疾为 8.1%。β 的分子特征显示所有 HbS 病例均存在阿拉伯-印度单倍型,所有β-地中海贫血病例均存在 IVS 1-5 G→C 突变。在α-地中海贫血病例中,αα/α-3.7 基因缺失最为常见(38%),其次是αα/α-4.2(18%)和α-3.7/α-3.7(4%)。发现 G6PD 奥里萨邦(131C→G)突变的频率为 97.9%,G6PD 地中海(563C→T)为 2.1%。约 57.4%的 G6PD 缺乏症患者和 16%的 AS 患者疟疾检测呈阳性。
本研究揭示了在所研究人群中广泛存在镰状细胞性贫血、α-地中海贫血、G6PD 缺乏症和疟疾。G6PD 缺乏症和疟疾的中高度流行率需要在使用伯氨喹(PQ)进行根治性治疗之前对 PVTGs 进行 G6PD 检测。奥里萨邦的 PVTGs 需要进行 HbS 的筛查和咨询。