Roux Alexia, David Valentin, Bardet M Sylvia, Auditeau Emilie, Durand Fontanier Sylvaine, Taibi Abdelkader
Visceral Surgery Department, Limoges University Hospital, Limoges, France.
University Limoges, Limoges, France.
Front Oncol. 2022 Oct 25;12:943522. doi: 10.3389/fonc.2022.943522. eCollection 2022.
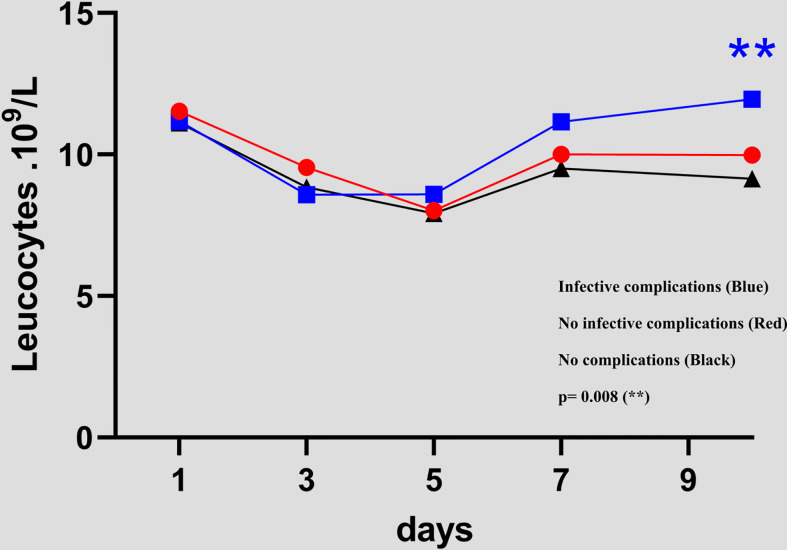
C-reactive protein (CRP), white blood cells and procalcitonin (PCT) participate in the systemic response to inflammation and increase after postoperative infective complications. Postoperative complications after CRS and HIPEC could be predicted using the CRP cut-off value (169 mg/L at PODs 3-5 and 62 mg/L at PODs 7-10).
Postoperative elevation of C-reactive protein (CRP) can be used in order to predict the postoperative complications in many indications. Cytoreduction surgery (CRS) associated with hyperthermic intraperitoneal chemotherapy (HIPEC) is associated with high morbidity.
The aim of the study was to demonstrate the CRP predictive value for the occurrence of complications.
All patients who had CRS and HIPEC, regardless of the origin of peritoneal metastasis, were included in this retrospective study. Postoperative complications and CRP and white blood cell (WBC) counts were recorded from postoperative day (POD) 1 through 10.
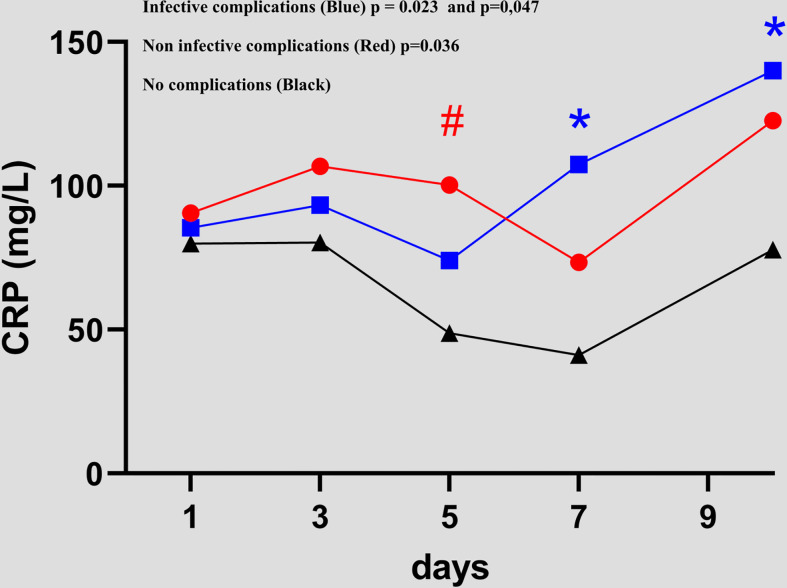
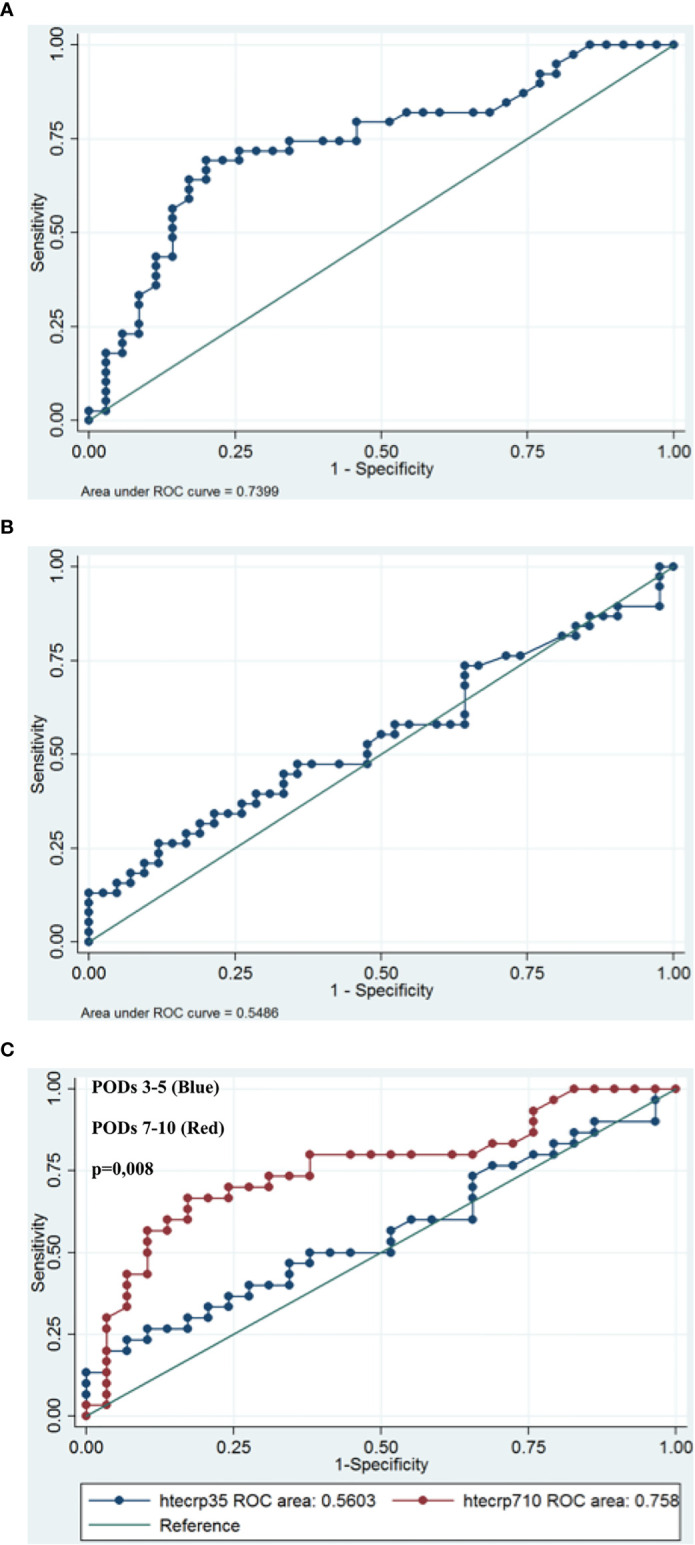
Among the 127 patients included, 58 (45.7%) had no complications (NCs), 53 (41.7%) had infective complications (ICs), and 16 (12.6%) had non-infective complications (NICs). The IC group had a higher CRP value than the NC group, which was statistically significant from POD7 to POD10 (41.1 versus 107.5 p = 0.023 and 77.8 versus 140 p = 0.047, respectively). A cut-off CRP value was 169 mg/L at PODs 3-5 and 62 mg/L at PODs 7-10. The area under the curve (AUC) at POD5 was 0.56 versus 0.76 at POD7, p=0.007. The sensibility, specificity, positive and negative predictive values of these cut-offs were 55%, 83%, 74% and 67%, respectively. Moreover, 17 patients (32%) with ICs had a CRP value higher than these cut-offs before the diagnosis was made by the medical team.
This study suggested that postoperative complications could be predicted using the CRP cut-off value on PODs 3-5 (169 mg/l) and PODs 7-10 (62 mg/l) after CRS and HIPEC.
C反应蛋白(CRP)、白细胞和降钙素原(PCT)参与全身炎症反应,在术后感染性并发症发生后会升高。使用CRP临界值(术后第3 - 5天为169 mg/L,术后第7 - 10天为62 mg/L)可预测CRS和HIPEC术后的并发症。
C反应蛋白(CRP)术后升高可用于预测多种情况下的术后并发症。细胞减灭术(CRS)联合热灌注化疗(HIPEC)的发病率较高。
本研究旨在证明CRP对并发症发生的预测价值。
本回顾性研究纳入了所有接受CRS和HIPEC的患者,无论腹膜转移的来源如何。记录术后第1天至第10天的术后并发症、CRP和白细胞(WBC)计数。
在纳入的127例患者中,58例(45.7%)无并发症(NCs),53例(41.7%)有感染性并发症(ICs),16例(12.6%)有非感染性并发症(NICs)。IC组的CRP值高于NC组,从术后第7天到第10天具有统计学意义(分别为41.1对107.5,p = 0.023;77.8对140,p = 0.047)。术后第3 - 5天的CRP临界值为169 mg/L,术后第7 - 10天为62 mg/L。术后第5天的曲线下面积(AUC)为0.56,术后第7天为0.76,p = 0.007。这些临界值的敏感性、特异性、阳性和阴性预测值分别为55%、83%、74%和67%。此外,17例(32%)有ICs的患者在医疗团队做出诊断之前CRP值就高于这些临界值。
本研究表明,使用CRS和HIPEC术后第3 - 5天(169 mg/l)和第7 - 10天(62 mg/l)的CRP临界值可预测术后并发症。