Cardiovascular Department, Azienda Sanitaria Universitaria Giuliano Isontina (ASUGI), University of Trieste (a member of the European Reference Network for rare, low-prevalence, or complex diseases of the Heart [ERN GUARD-Heart]), Trieste, Italy.
Cardiovascular Department, Azienda Sanitaria Universitaria Giuliano Isontina (ASUGI), University of Trieste (a member of the European Reference Network for rare, low-prevalence, or complex diseases of the Heart [ERN GUARD-Heart]), Trieste, Italy.
J Am Coll Cardiol. 2022 Nov 22;80(21):1981-1994. doi: 10.1016/j.jacc.2022.08.804.
Diverse genetic backgrounds often lead to phenotypic heterogeneity in cardiomyopathies (CMPs). Previous genotype-phenotype studies have primarily focused on the analysis of a single phenotype, and the diagnostic and prognostic features of the CMP genotype across different phenotypic expressions remain poorly understood.
We sought to define differences in outcome prediction when stratifying patients based on phenotype at presentation compared with genotype in a large cohort of patients with CMPs and positive genetic testing.
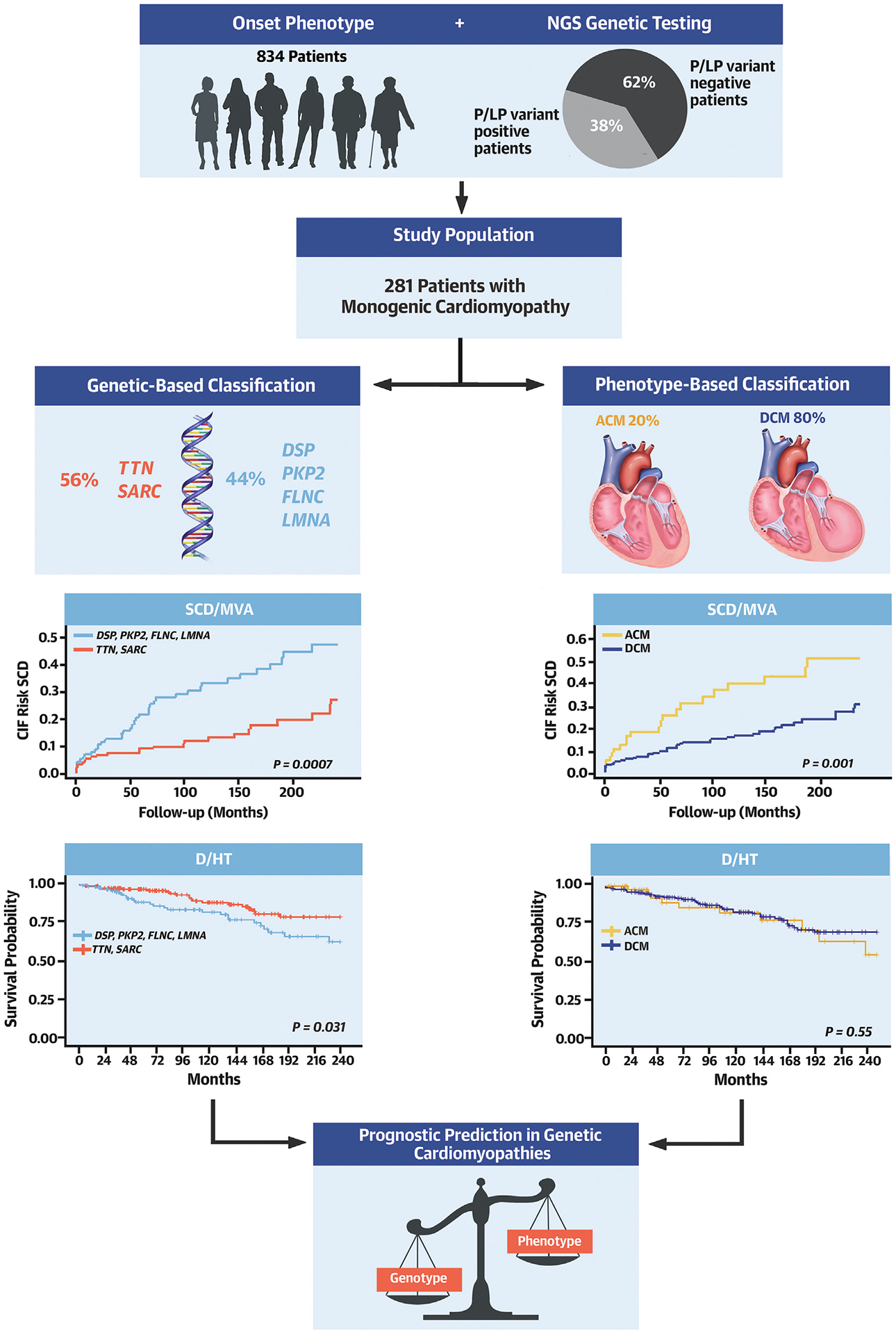
Dilated cardiomyopathy (DCM), arrhythmogenic right ventricular cardiomyopathy, left-dominant arrhythmogenic cardiomyopathy, and biventricular arrhythmogenic cardiomyopathy were examined in this study. A total of 281 patients (80% DCM) with pathogenic or likely pathogenic variants were included. The primary and secondary outcomes were: 1) all-cause mortality (D)/heart transplant (HT); 2) sudden cardiac death/major ventricular arrhythmias (SCD/MVA); and 3) heart failure-related death (DHF)/HT/left ventricular assist device implantation (LVAD).
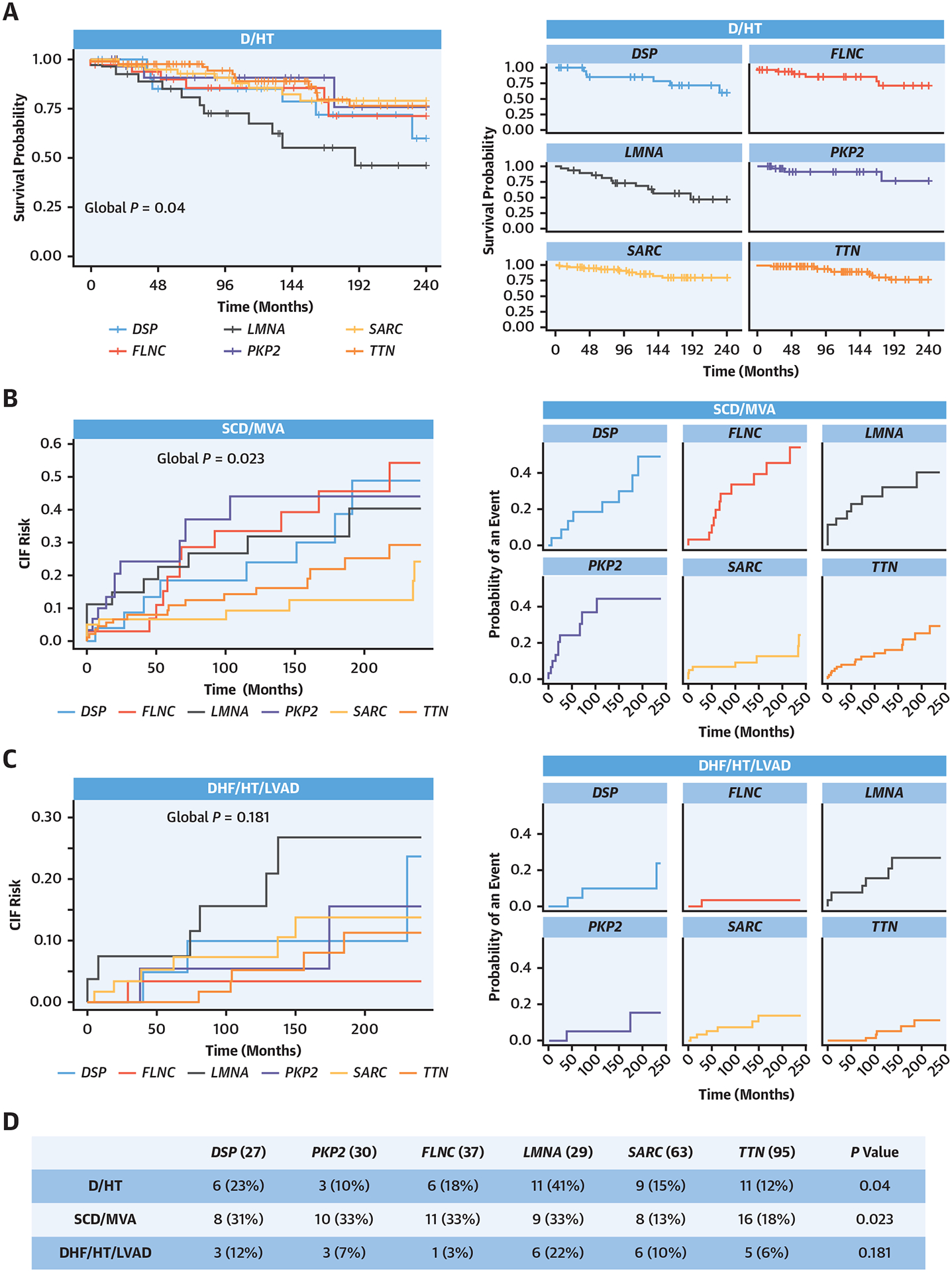
Survival analysis revealed that SCD/MVA events occurred more frequently in patients without a DCM phenotype and in carriers of DSP, PKP2, LMNA, and FLNC variants. However, after adjustment for age and sex, genotype-based classification, but not phenotype-based classification, was predictive of SCD/MVA. LMNA showed the worst trends in terms of D/HT and DHF/HT/LVAD.
Genotypes were associated with significant phenotypic heterogeneity in genetic cardiomyopathies. Nevertheless, in our study, genotypic-based classification showed higher precision in predicting the outcome of patients with CMP than phenotype-based classification. These findings add to our current understanding of inherited CMPs and contribute to the risk stratification of patients with positive genetic testing.
不同的遗传背景常常导致心肌病(CMP)的表型异质性。先前的基因型-表型研究主要集中于单一表型的分析,而不同表型表达的 CMP 基因型的诊断和预后特征仍知之甚少。
我们旨在通过对携带致病性或可能致病性变异的 281 名 CMP 患者(80%为扩张型心肌病)进行研究,比较基于表型和基因型分层的患者在预后预测方面的差异。
本研究检查了扩张型心肌病(DCM)、致心律失常性右心室心肌病、左优势型致心律失常性心肌病和双心室致心律失常性心肌病。主要和次要结局为:1)全因死亡率(D)/心脏移植(HT);2)心源性猝死/主要室性心律失常(SCD/MVA);3)心力衰竭相关死亡(DHF)/HT/左心室辅助装置植入(LVAD)。
生存分析显示,无 DCM 表型的患者和携带 DSP、PKP2、LMNA 和 FLNC 变异的患者更常发生 SCD/MVA 事件。然而,在校正年龄和性别后,基于基因型的分类,而不是基于表型的分类,是 SCD/MVA 的预测因素。LMNA 在 D/HT 和 DHF/HT/LVAD 方面表现出最差的趋势。
基因型与遗传型 CMP 中的显著表型异质性相关。然而,在我们的研究中,基于基因型的分类在预测 CMP 患者的预后方面比基于表型的分类具有更高的准确性。这些发现增加了我们对遗传性 CMP 的理解,并有助于对阳性基因检测患者进行风险分层。